

Dosimetric validation of a magnetic resonance image gated radiotherapy system using a motion phantom and radiochromic film
- PMID: 28436094
- PMCID: PMC5689863
- DOI: 10.1002/acm2.12088
Dosimetric validation of a magnetic resonance image gated radiotherapy system using a motion phantom and radiochromic film
Abstract
Purpose: Magnetic resonance image (MRI) guided radiotherapy enables gating directly on the target position. We present an evaluation of an MRI-guided radiotherapy system's gating performance using an MRI-compatible respiratory motion phantom and radiochromic film. Our evaluation is geared toward validation of our institution's clinical gating protocol which involves planning to a target volume formed by expanding 5 mm about the gross tumor volume (GTV) and gating based on a 3 mm window about the GTV.
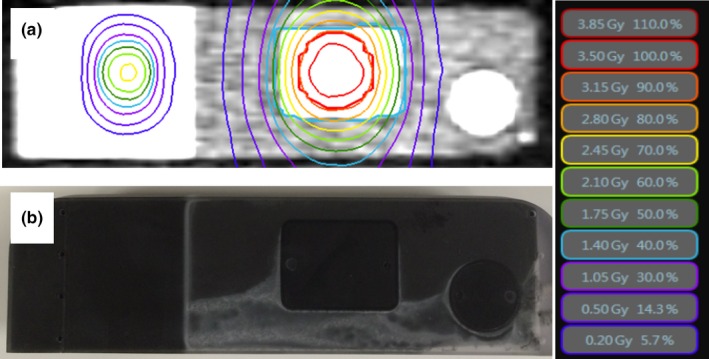
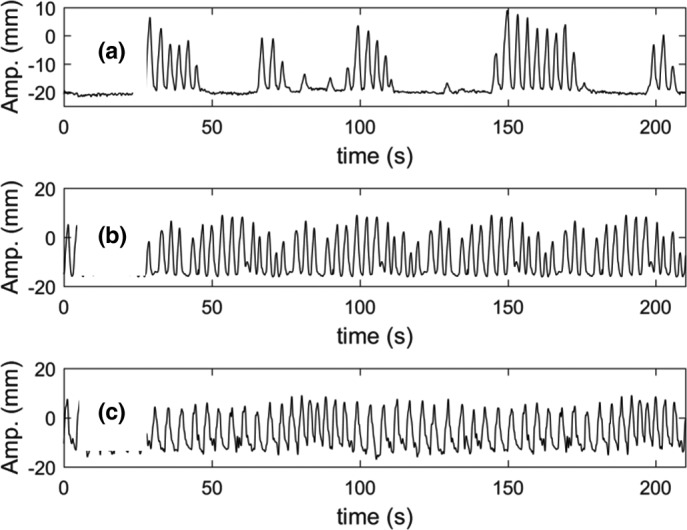
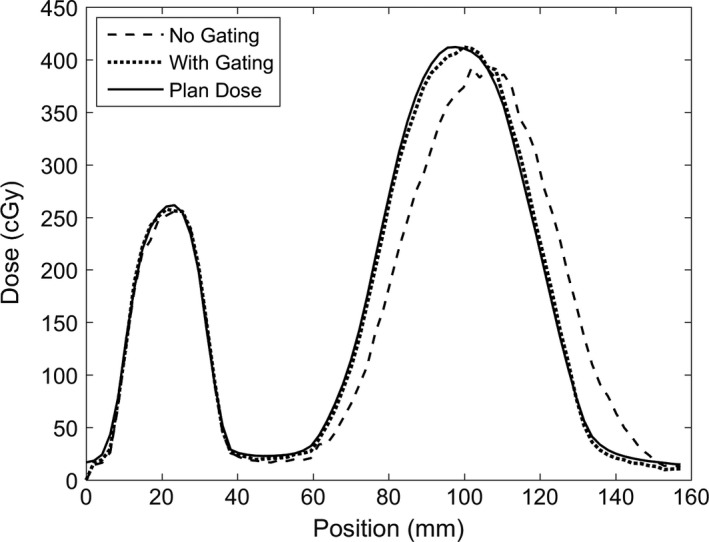
Methods: The motion phantom consisted of a target rod containing high-contrast target inserts which moved in the superior-inferior direction inside a body structure containing background contrast material. The target rod was equipped with a radiochromic film insert. Treatment plans were generated for a 3 cm diameter spherical planning target volume, and delivered to the phantom at rest and in motion with and without gating. Both sinusoidal trajectories and tumor trajectories measured during MRI-guided treatments were used. Similarity of the gated dose distribution to the planned, motion-frozen, distribution was quantified using the gamma technique.
Results: Without gating, gamma pass rates using 4%/3 mm criteria were 22-59% depending on motion trajectory. Using our clinical standard of repeated breath holds and a gating window of 3 mm with 10% target allowed outside the gating boundary, the gamma pass rate was 97.8% with 3%/3 mm gamma criteria. Using a 3 mm window and 10% allowed excursion, all of the patient tumor motion trajectories at actual speed resulting in at least 95% gamma pass rate at 4%/3 mm.
Conclusions: Our results suggest that the device can be used to compensate respiratory motion using a 3 mm gating margin and 10% allowed excursion results in conjunction with repeated breath holds. Full clinical validation requires a comprehensive evaluation of tracking performance in actual patient images, outside the scope of this study.
Keywords: MRI; motion management; quality assurance; radiotherapy.
© 2017 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Figures

References
-
- Keall PJ, Mageras GS, Balter JM, et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med Phys. 2006;33:3874–3900. - PubMed
-
- Wagman R, Yorke E, Ford E, et al. Respiratory gating for liver tumors: Use in dose escalation. Int J Radiat Oncol Biol Phys. 2003;55:659–668. - PubMed
-
- Giraud P, Yorke E, Ford EC, et al. Reduction of organ motion in lung tumors with respiratory gating. Lung Cancer. 2006;51:41–51. - PubMed
-
- Kini VR, Vedam SS, Keall PJ, Patil S, Chen C, Mohan R. Patient training in respiratory‐gated radiotherapy. Med Dosim. 2003;28:7–11. - PubMed
-
- Shirato H, Shimizu S, Kunieda T, et al. Physical aspects of a real‐time tumor‐tracking system for gated radiotherapy. Int J Radiat Oncol Biol Phys. 2000;48:1187–1195. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
