

A hemorrhagic complication after Onyx embolization of a tentorial dural arteriovenous fistula: A caution about subdural extension with pial arterial supply
- PMID: 28436714
- PMCID: PMC5490865
- DOI: 10.1177/1591019917694839
A hemorrhagic complication after Onyx embolization of a tentorial dural arteriovenous fistula: A caution about subdural extension with pial arterial supply
Abstract
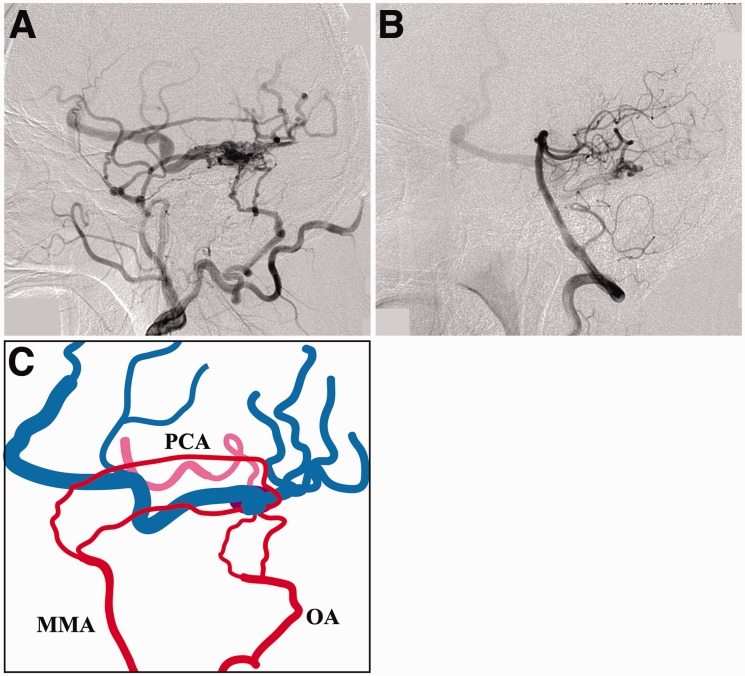
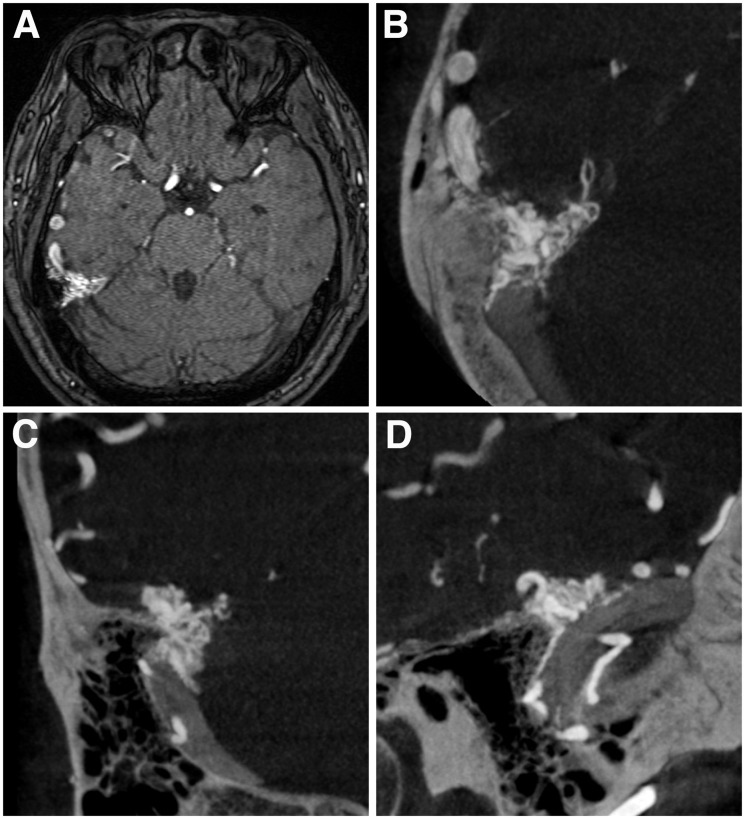
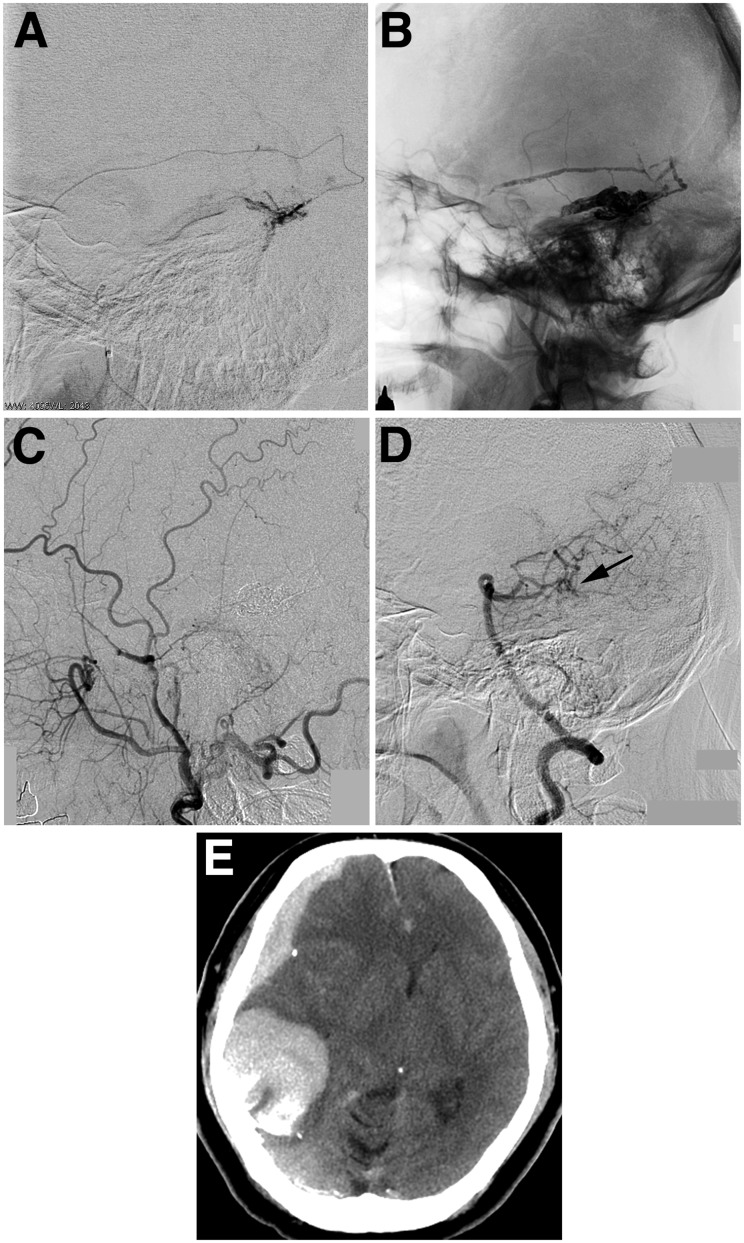
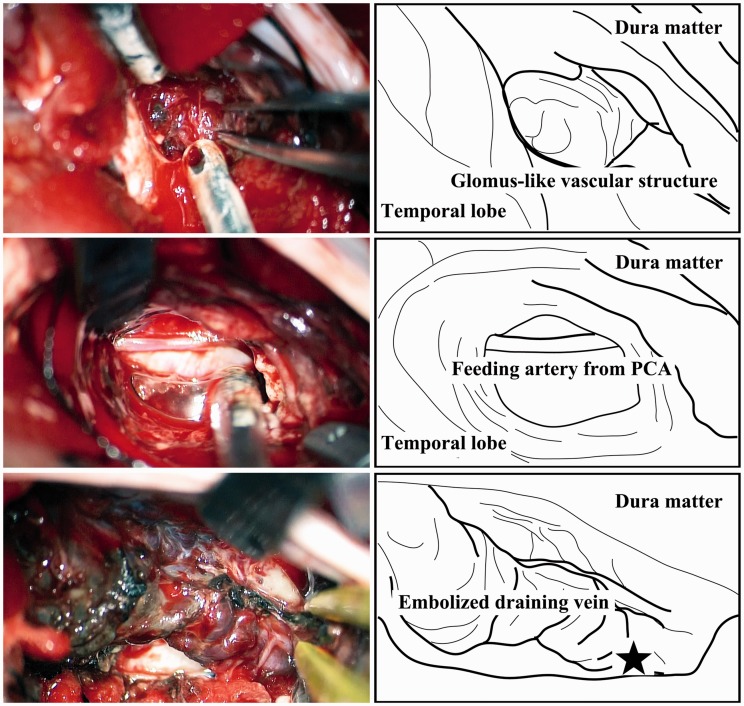
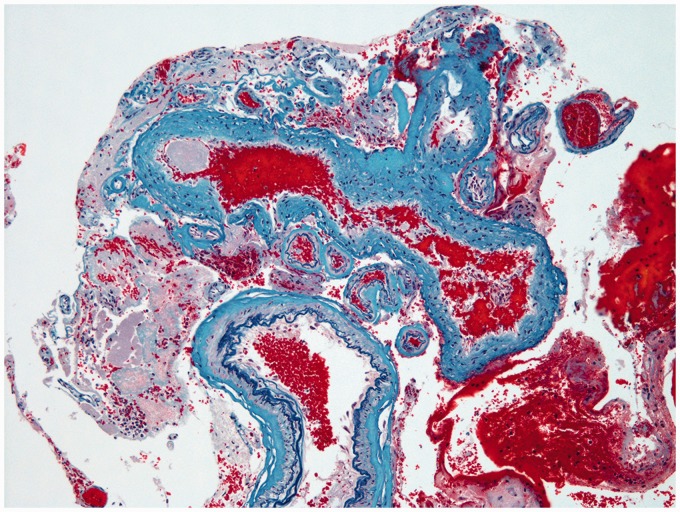
We report a case of tentorial dural arteriovenous fistula (DAVF) with a severe intracranial hemorrhage occurring after Onyx embolization. A 40-year-old man presented with an asymptomatic tentorial DAVF on angiography. Transarterial embolization with Onyx was performed via the middle meningeal artery, and the cast filled the fistula itself and its proximal draining vein. Postoperative angiography confirmed complete occlusion of the DAVF. A computed tomography scan performed immediately after the procedure demonstrated an acute subdural hematoma with the temporal hemorrhage. Emergency craniotomy revealed continuous arterial bleeding from a viable glomus-like vascular structure around the proximal part of the embolized draining vein, fed by a pial artery arising from the posterior cerebral artery. Pathologic findings suggested diagnosis of vascular malformation extending into the subdural space. Tentorial DAVFs can extend to the subdural space along their drainage route, and may be involved in severe hemorrhagic complications of curative endovascular treatment using Onyx, particularly those with pial arterial supply.
Keywords: Dural arteriovenous fistula; Onyx; endovascular treatment; hemorrhage.
Figures
References
-
- Miller TR, Gandhi D. Intracranial dural arteriovenous fistulae: Clinical presentation and management strategies. Stroke 2015; 46: 2017–2025. - PubMed
-
- Bulters DO, Mathad N, Culliford D, et al. The natural history of cranial dural arteriovenous fistulae with cortical venous reflux—the significance of venous ectasia. Neurosurgery 2012; 70: 312–318. - PubMed
-
- Youssef PP, Schuette AJ, Cawley CM, et al. Advances in surgical approaches to dural fistulas. Neurosurgery 2014; 74: 532–541. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
