

Both Positive and Negative Fluid Balance May Be Associated With Reduced Long-Term Survival in the Critically Ill
- PMID: 28437375
- PMCID: PMC5511076
- DOI: 10.1097/CCM.0000000000002372
Both Positive and Negative Fluid Balance May Be Associated With Reduced Long-Term Survival in the Critically Ill
Abstract
Objectives: Among critically ill patients with acute kidney injury, exposure to positive fluid balance, compared with negative fluid balance, has been associated with mortality and impaired renal recovery. However, it is unclear whether positive and negative fluid balances are associated with poor outcome compared to patients with even fluid balance (euvolemia). In this study, we examined the association between exposure to positive or negative fluid balance, compared with even fluid balance, on 1-year mortality and renal recovery.
Design: Retrospective cohort study.
Setting: Eight medical-surgical ICUs at the University of Pittsburgh Medical Center, Pittsburgh, PA.
Patients: Critically ill patients admitted between July 2000 and October 2008.
Interventions: None.
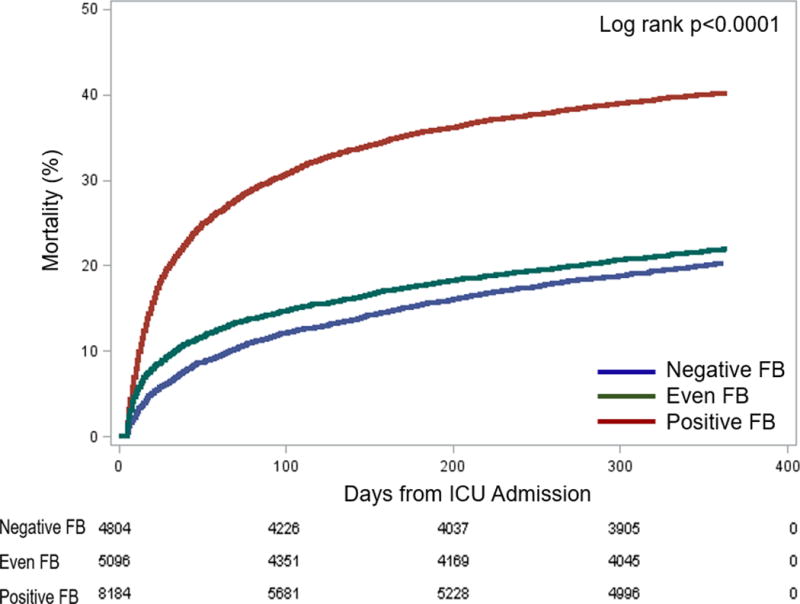
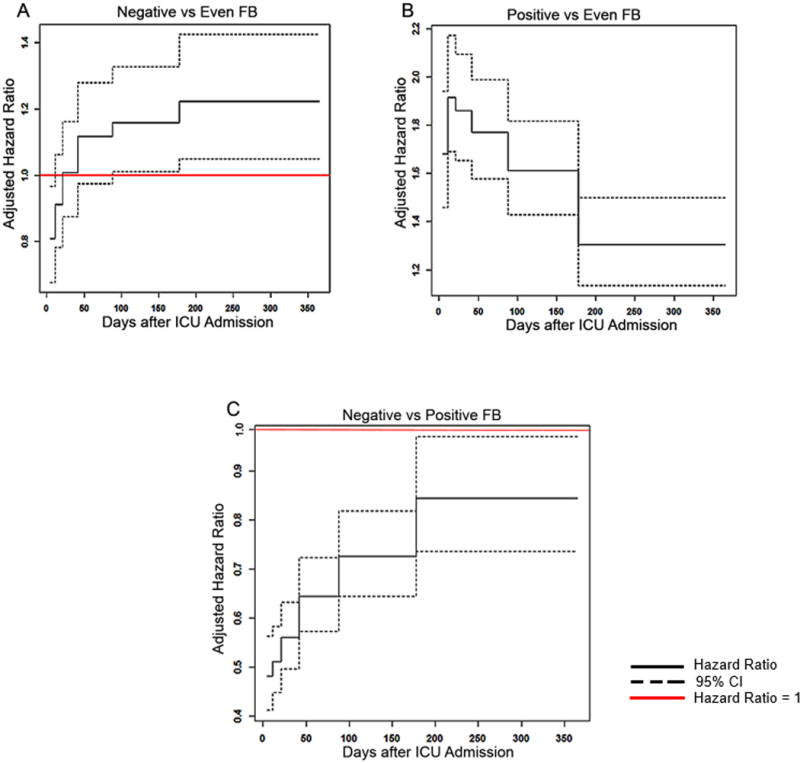
Measurements and main results: Among 18,084 patients, fluid balance was categorized as negative (< 0%), even (0% to < 5%), or positive (≥ 5%). Following propensity matching, positive fluid balance, compared with even or negative fluid balance, was associated with increased mortality (30.3% vs 21.1% vs 22%, respectively; p < 0.001). Using Gray's model, negative fluid balance, compared with even fluid balance, was associated with lower short-term mortality (adjusted hazard ratio range, 0.81; 95% CI, 0.68-0.96) but higher long-term mortality (adjusted hazard ratio range, 1.16-1.22; p = 0.004). Conversely, positive fluid balance was associated with higher mortality throughout 1-year (adjusted hazard ratio range, 1.30-1.92; p < 0.001), which was attenuated in those who received renal replacement therapy (positive fluid balance × renal replacement therapy interaction (adjusted hazard ratio range, 0.43-0.89; p < 0.001). Of patients receiving renal replacement therapy, neither positive (adjusted odds ratio, 0.98; 95% CI, 0.68-1.4) nor negative (adjusted odds ratio, 0.81; 95% CI, 0.43-1.55) fluid balance was associated with renal recovery.
Conclusions: Among critically ill patients, exposure to positive or negative fluid balance, compared with even fluid balance, was associated with higher 1-year mortality. This mortality risk associated with positive fluid balance, however, was attenuated by use of renal replacement therapy. We found no association between fluid balance and renal recovery.
Conflict of interest statement
Figures
References
-
- Lowell JA, Schifferdecker C, Driscoll DF, et al. Postoperative fluid overload: not a benign problem. Critical care medicine. 1990;18(7):728–733. - PubMed
-
- Goldstein SL, Currier H, Graf JM, et al. Outcome in children receiving continuous venovenous hemofiltration. Pediatrics. 2001;107(6):1309–1312. - PubMed
-
- National Heart L, Blood Institute Acute Respiratory Distress Syndrome Clinical Trials N. Wiedemann HP, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564–2575. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
