

Normothermic Perfusion in the Assessment and Preservation of Declined Livers Before Transplantation: Hyperoxia and Vasoplegia-Important Lessons From the First 12 Cases
- PMID: 28437389
- PMCID: PMC5642347
- DOI: 10.1097/TP.0000000000001661
Normothermic Perfusion in the Assessment and Preservation of Declined Livers Before Transplantation: Hyperoxia and Vasoplegia-Important Lessons From the First 12 Cases
Abstract
Background: A program of normothermic ex situ liver perfusion (NESLiP) was developed to facilitate better assessment and use of marginal livers, while minimizing cold ischemia.
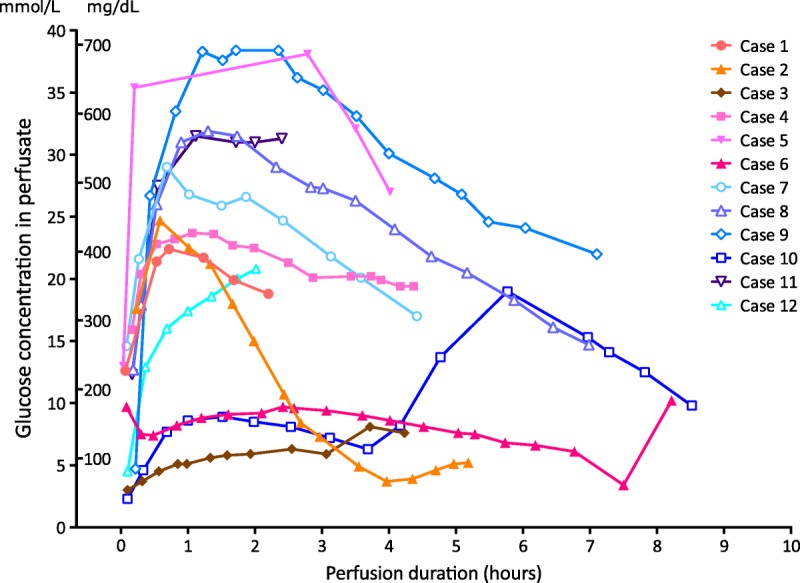
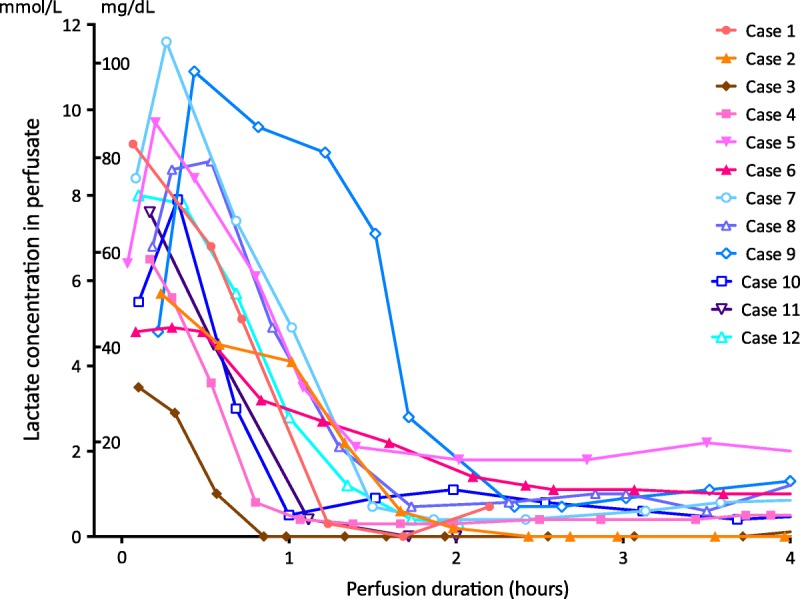
Methods: Declined marginal livers and those offered for research were evaluated. Normothermic ex situ liver perfusion was performed using an erythrocyte-based perfusate. Viability was assessed with reference to biochemical changes in the perfusate.
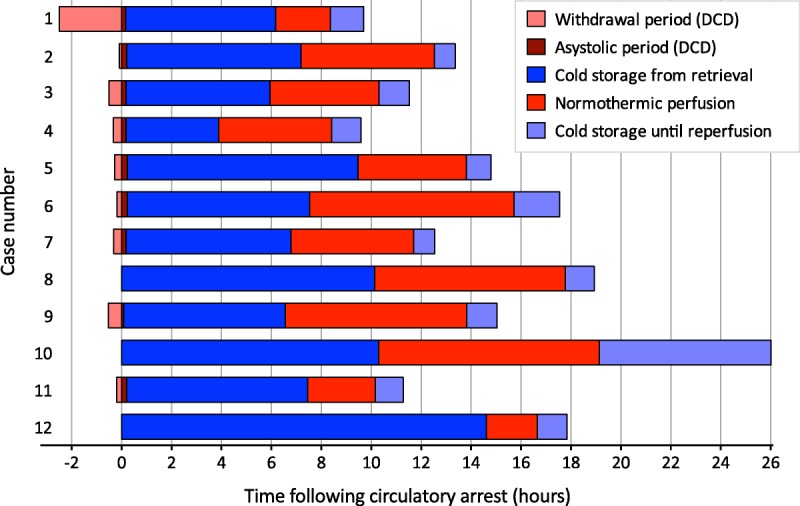
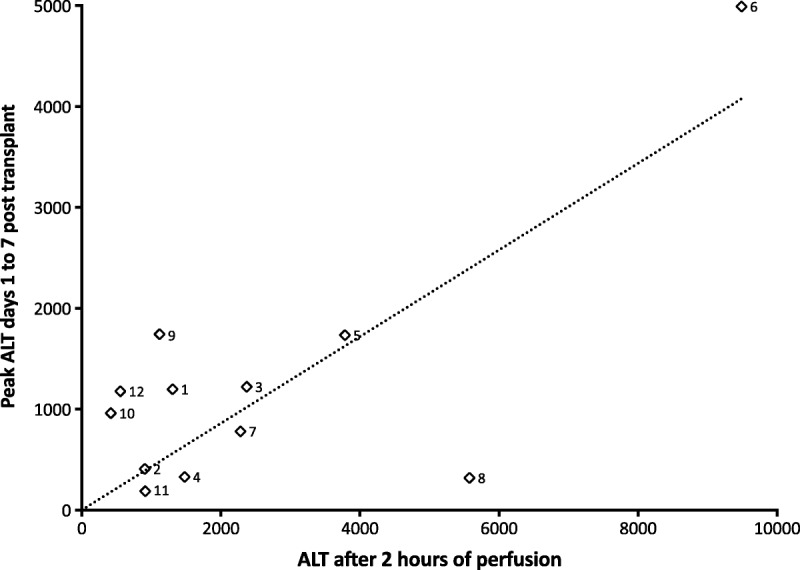
Results: Twelve livers (9 donation after circulatory death [DCD] and 3 from brain-dead donors), median Donor Risk Index 2.15, were subjected to NESLiP for a median 284 minutes (range, 122-530 minutes) after an initial cold storage period of 427 minutes (range, 222-877 minutes). The first 6 livers were perfused at high perfusate oxygen tensions, and the subsequent 6 at near-physiologic oxygen tensions. After transplantation, 5 of the first 6 recipients developed postreperfusion syndrome and 4 had sustained vasoplegia; 1 recipient experienced primary nonfunction in conjunction with a difficult explant. The subsequent 6 liver transplants, with livers perfused at lower oxygen tensions, reperfused uneventfully. Three DCD liver recipients developed cholangiopathy, and this was associated with an inability to produce an alkali bile during NESLiP.
Conclusions: Normothermic ex situ liver perfusion enabled assessment and transplantation of 12 livers that may otherwise not have been used. Avoidance of hyperoxia during perfusion may prevent postreperfusion syndrome and vasoplegia, and monitoring biliary pH, rather than absolute bile production, may be important in determining the likelihood of posttransplant cholangiopathy. Normothermic ex situ liver perfusion has the potential to increase liver utilization, but more work is required to define factors predicting good outcomes.
Conflict of interest statement
A.B. is a joint holder of a patent on the design of the perfusion circuit used by the OrganOx Metra liver perfusion device. L.R. is now an employee of OrganOx. The other authors declare no other conflicts of interest.
Figures




References
-
- Kim WR, Lake JR, Smith JM, et al. OPTN/SRTR 2014 annual data report: liver. Am J Transplant. 2016;16(Supp. 2):69–98. - PubMed
-
- NHS Blood and Transplant. Annual Report on Liver Transplantation. Report for 2014/15. <http://www.odt.nhs.uk/pdf/organ_specific_report_liver_2015.pdf> Published 2015. Accessed 28th March 2016.
-
- NHS Blood and Transplant. Organ donation and Transplantation Activity Report 2014/15. <http://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pd...> Published 2015. Accessed 28th March 2016.
-
- NHS Blood and Transplant. Policy POL196/4.1 Deceased Donor Liver Distribution and Allocation. <http://www.odt.nhs.uk/pdf/liver_allocation_policy.pdf> Published 2015. Accessed 28th March 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
