

Clinical Aspects of Glucose Transporter Type 1 Deficiency: Information From a Global Registry
- PMID: 28437535
- PMCID: PMC5822202
- DOI: 10.1001/jamaneurol.2017.0298
Clinical Aspects of Glucose Transporter Type 1 Deficiency: Information From a Global Registry
Abstract
Importance: Case reports regularly document unique or unusual aspects of glucose transporter type 1 deficiency (G1D). In contrast, population studies from which to draw global inferences are lacking. Twenty-five years after the earliest case reports, this deficiency still particularly affects treatment and prognostic counseling.
Objective: To examine the most common features of G1D.
Design, setting, and participants: In this study, data were collected electronically from 181 patients with G1D through a web-based, worldwide patient registry from December 1, 2013, through December 1, 2016. The study used several statistical methods tailored to address the age at onset of various forms of G1D, associated manifestations, natural history, treatment efficacy, and diagnostic procedures. These factors were correlated in a predictive mathematical model designed to guide prognosis on the basis of clinical features present at diagnosis.
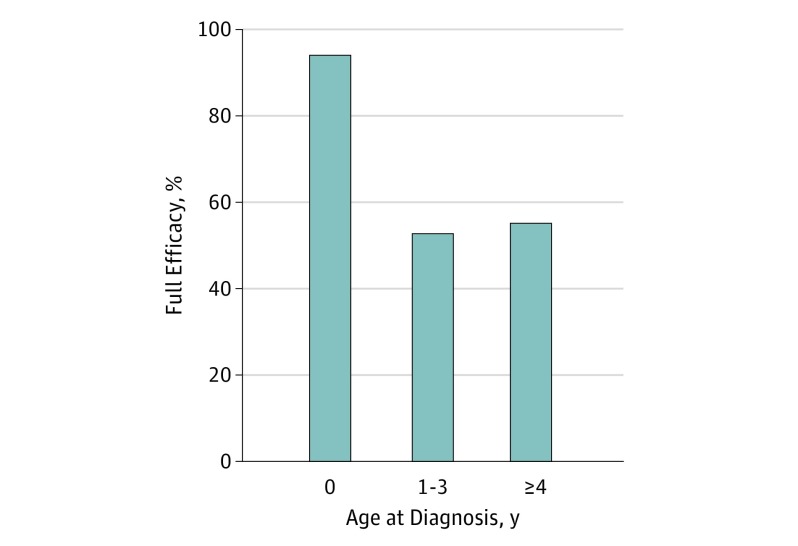
Results: A total of 181 patients with G1D were included in the study (92 [50.8%] male and 89 female [49.2%]; median age, 9 years; age range, 0-65 years). As previously known, a relatively large variety of common phenotypes are characteristic of the G1D syndrome, including movement disorders, absence epilepsy (typical and atypical), and myoclonic and generalized epilepsies. The 3 main novel results are (1) the feasibility of effective dietary therapies (such as the modified Atkins diet) other than the ketogenic diet, (2) the relatively frequent occurrence (one-fourth of cases) of white matter magnetic resonance imaging abnormalities, and (3) the favorable effect of early diagnosis and treatment regardless of treatment modality and mutation type. In fact, the most important factor that determines outcome is age at diagnosis, as reflected in a predictive mathematical model.
Conclusions and relevance: The results reveal several changing notions in the approach to G1D syndrome diagnosis and treatment, such as the perceived absolute requirement for a ketogenic diet, the assumed lack of structural brain defects, and the potential existence of genotype-phenotype correlations, all of which are contested by the registry data.
Conflict of interest statement
Figures
References
-
- Arsov T, Mullen SA, Rogers S, et al. Glucose transporter 1 deficiency in the idiopathic generalized epilepsies. Ann Neurol. 2012;72(5):807-815. - PubMed
-
- Arsov T, Mullen SA, Damiano JA, et al. Early onset absence epilepsy: 1 in 10 cases is caused by GLUT1 deficiency. Epilepsia. 2012;53(12):e204-e207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
