

Accuracy of serum procalcitonin for the diagnosis of sepsis in neonates and children with systemic inflammatory syndrome: a meta-analysis
- PMID: 28438138
- PMCID: PMC5404674
- DOI: 10.1186/s12879-017-2396-7
Accuracy of serum procalcitonin for the diagnosis of sepsis in neonates and children with systemic inflammatory syndrome: a meta-analysis
Abstract
Background: A number of biomarkers have been studied for the diagnosis of sepsis in paediatrics, but no gold standard has been identified. Procalcitonin (PCT) was demonstrated to be an accurate biomarker for the diagnosis of sepsis in adults and showed to be promising in paediatrics. Our study reviewed the diagnostic accuracy of PCT as an early biomarker of sepsis in neonates and children with suspected sepsis.
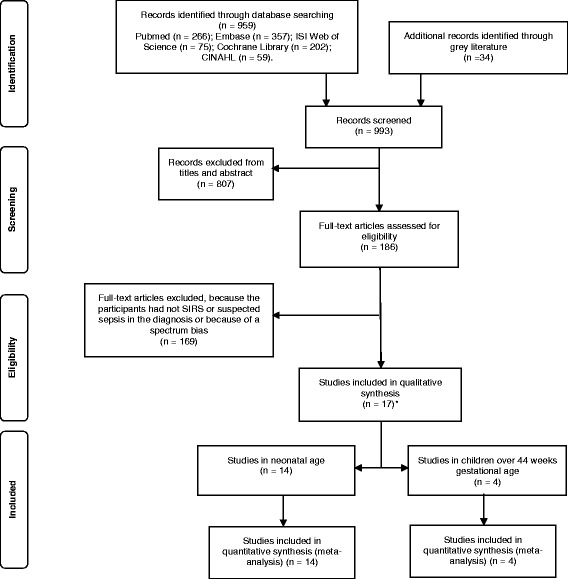
Methods: A comprehensive literature search was carried out in Medline/Pubmed, Embase, ISI Web of Science, CINAHL and Cochrane Library, for studies assessing PCT accuracy in the diagnosis of sepsis in children and neonates with suspected sepsis. Studies in which the presence of infection had been confirmed microbiologically or classified as "probable" by chart review were included. Studies comparing patients to healthy subjects were excluded. We analysed data on neonates and children separately. Our primary outcome was the diagnostic accuracy of PCT at the cut-off of 2-2.5 ng/ml, while as secondary outcomes we analysed PCT cut-offs <2 ng/ml and >2.5 ng/ml. Pooled sensitivities and specificities were calculated by a bivariate meta-analysis and heterogeneity was graphically evaluated.
Results: We included 17 studies, with a total of 1408 patients (1086 neonates and 322 children). Studies on neonates with early onset sepsis (EOS) and late onset sepsis (LOS) were grouped together. In the neonatal group, we calculated a sensitivity of 0.85, confidence interval (CI) (0.76; 0.90) and specificity of 0.54, CI (0.38; 0.70) at the PCT cut-off of 2.0-2.5 ng/ml. In the paediatric group it was not possible to undertake a pooled analysis at the PCT cut-off of 2.0-2.5 ng/ml, due to the paucity of the studies.
Conclusions: PCT shows a moderate accuracy for the diagnosis of sepsis in neonates with suspected sepsis at the cut-off of 2.0-2.5 ng/ml. More studies with high methodological quality are warranted, particularly in neonates, studies considering EOS and LOS separately are needed to improve specificity.
Trial registration: PROSPERO Identifier: CRD42016033809 . Registered 30 Jan 2016.
Keywords: Biological markers; Child; Infant; Meta-analysis; Procalcitonin; Sepsis; Systemic inflammatory response syndrome.
Figures
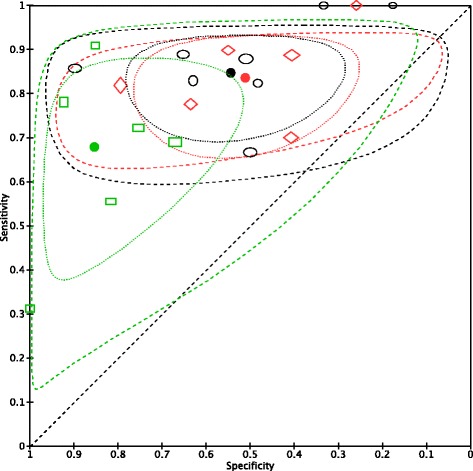
 PCT neon – cut-off <2
PCT neon – cut-off <2  PCT neon – cut-off > 2.5
PCT neon – cut-off > 2.5  PCT neon – cut-off =2/2.5
PCT neon – cut-off =2/2.5
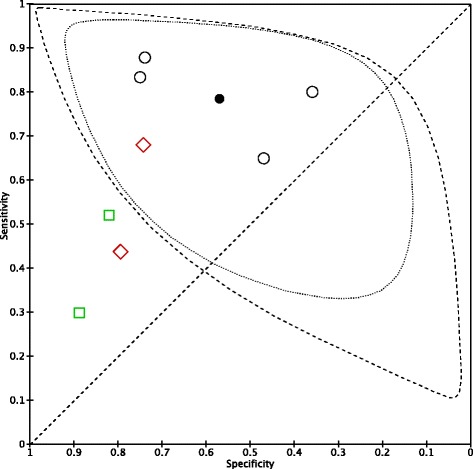
 PCT paed – cut-off <2
PCT paed – cut-off <2  PCT paed – cut-off > 2.5
PCT paed – cut-off > 2.5  PCT paed – cut-off =2/2.5
PCT paed – cut-off =2/2.5
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA. 2016;315(8):801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Goldstein B, Giroir B, Randolph A. International consensus conference on Paediatric sepsis: international paediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in paediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi: 10.1097/01.PCC.0000149131.72248.E6. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
