

Significant Radiologic Response of Pancreatic Metastasis After Targeted Therapy of Ceritinib (LDK378) for ALK-Rearranged Lung Adenocarcinoma Presenting With Hyperglycemia
- PMID: 28438234
- PMCID: PMC7841023
- DOI: 10.3727/096504016X14801968368898
Significant Radiologic Response of Pancreatic Metastasis After Targeted Therapy of Ceritinib (LDK378) for ALK-Rearranged Lung Adenocarcinoma Presenting With Hyperglycemia
Abstract
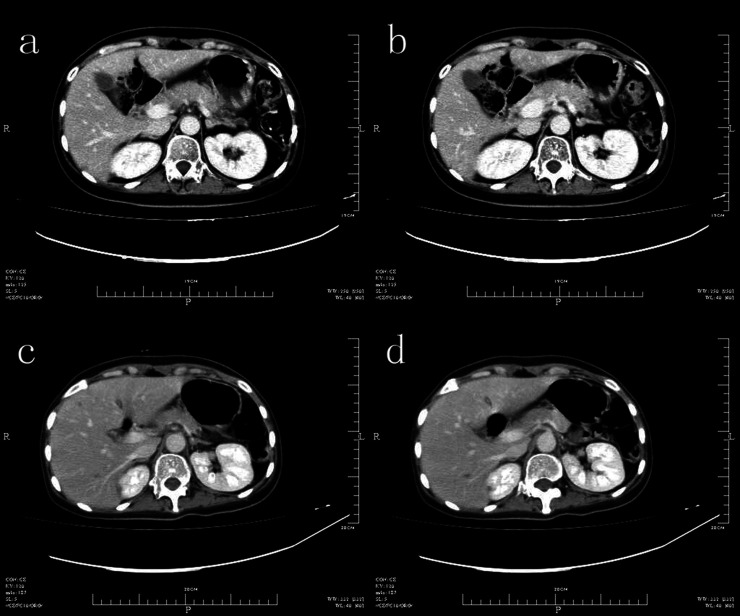
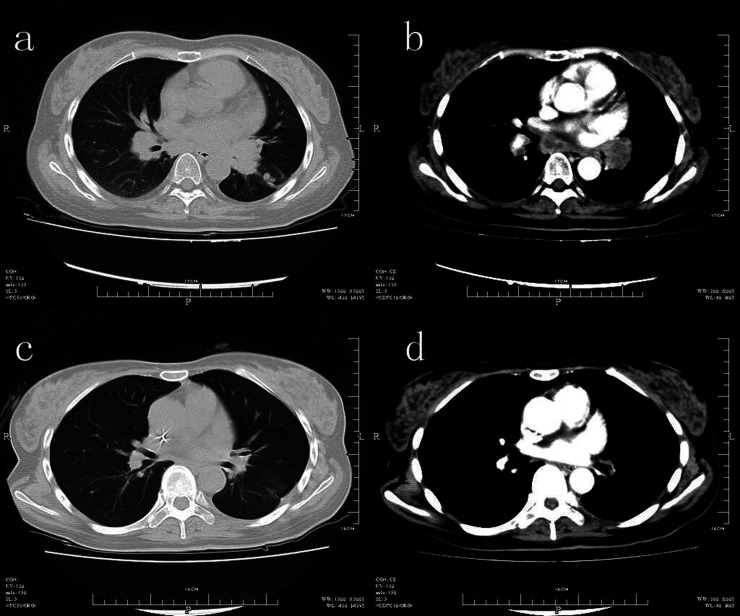
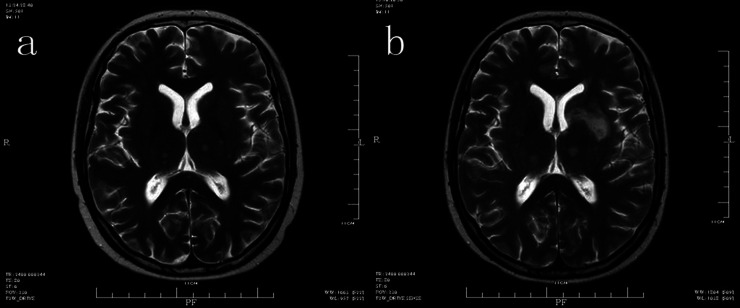
Pancreatic metastasis from non-small cell lung cancer (NSCLC) is usually asymptomatic or presents with abdominal pain, acute pancreatitis, or jaundice. A lung primary is associated with worse survival compared to pancreatic metastases from other organs. Surgical treatment of solitary metastasis to the pancreas from NSCLC has been reviewed in several studies, one of which had a notable disease-free interval. To our knowledge, there are no prior reports of targeted therapy of pancreatic metastasis of NSCLC followed by a significant response. Herein we report the case of a 31-year-old female with a solitary pancreatic metastasis from ALK-rearranged lung adenocarcinoma despite treatment with chemotherapy and crizotinib; she presented with symptoms of hyperglycemia. Targeted therapy with ceritinib (LDK378) led to symptomatic improvement and a significant radiologic response in the lung and pancreas, but not in the brain.
Figures
Similar articles
-
Ceritinib versus chemotherapy in patients with ALK-rearranged non-small-cell lung cancer previously given chemotherapy and crizotinib (ASCEND-5): a randomised, controlled, open-label, phase 3 trial.Lancet Oncol. 2017 Jul;18(7):874-886. doi: 10.1016/S1470-2045(17)30339-X. Epub 2017 Jun 9. Lancet Oncol. 2017. PMID: 28602779 Clinical Trial.
-
P-glycoprotein Mediates Ceritinib Resistance in Anaplastic Lymphoma Kinase-rearranged Non-small Cell Lung Cancer.EBioMedicine. 2015 Dec 12;3:54-66. doi: 10.1016/j.ebiom.2015.12.009. eCollection 2016 Jan. EBioMedicine. 2015. PMID: 26870817 Free PMC article.
-
K-RAS mutations indicating primary resistance to crizotinib in ALK-rearranged adenocarcinomas of the lung: Report of two cases and review of the literature.Lung Cancer. 2016 Mar;93:55-8. doi: 10.1016/j.lungcan.2016.01.002. Epub 2016 Jan 11. Lung Cancer. 2016. PMID: 26898615 Review.
-
Crizotinib primary resistance overcome by ceritinib in a patient with ALK-rearranged non-small cell lung cancer.Tumori. 2016 Nov 11;102(Suppl. 2). doi: 10.5301/tj.5000520. Tumori. 2016. PMID: 27197808
-
Molecular and clinical features of second-generation anaplastic lymphoma kinase inhibitors: ceritinib.Future Oncol. 2017 Dec;13(29):2629-2644. doi: 10.2217/fon-2017-0262. Epub 2017 Sep 11. Future Oncol. 2017. PMID: 28891712 Review.
References
-
- Cubilla A. L.; Fitzgerald P. J. Cancer of the exocrine pancreas: The pathologic aspects. CA Cancer J. Clin. 35(1):2–18; 1985. - PubMed
-
- Nakamura E.; Shimizu M.; Itoh T.; Manabe T. Secondary tumors of the pancreas: Clinicopathological study of 103 autopsy cases of Japanese patients. Pathol. Int. 51:686–690; 2001. - PubMed
-
- Pan B.; Lee Y.; Rodriguez T.; Lee J.; Saif M. W. Secondary tumors of the pancreas: A case series. Anticancer Res. 32(4):1449–1452; 2012. - PubMed
-
- Olson M. T.; Wakely P. E. Jr.; Ali S. Z. Metastases to the pancreas diagnosed by fine-needle aspiration. Acta Cytol. 57(5):473–480; 2013. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical