

Use and Customization of Risk Scores for Predicting Cardiovascular Events Using Electronic Health Record Data
- PMID: 28438733
- PMCID: PMC5532984
- DOI: 10.1161/JAHA.116.003670
Use and Customization of Risk Scores for Predicting Cardiovascular Events Using Electronic Health Record Data
Abstract
Background: Clinicians who are using the Framingham Risk Score (FRS) or the American College of Cardiology/American Heart Association Pooled Cohort Equations (PCE) to estimate risk for their patients based on electronic health data (EHD) face 4 questions. (1) Do published risk scores applied to EHD yield accurate estimates of cardiovascular risk? (2) Are FRS risk estimates, which are based on data that are up to 45 years old, valid for a contemporary patient population seeking routine care? (3) Do the PCE make the FRS obsolete? (4) Does refitting the risk score using EHD improve the accuracy of risk estimates?
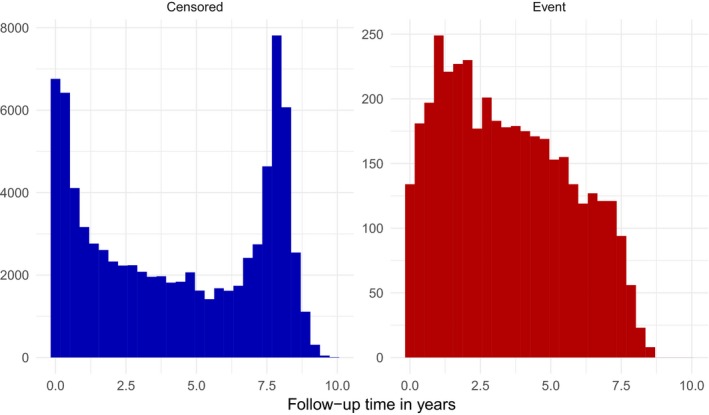
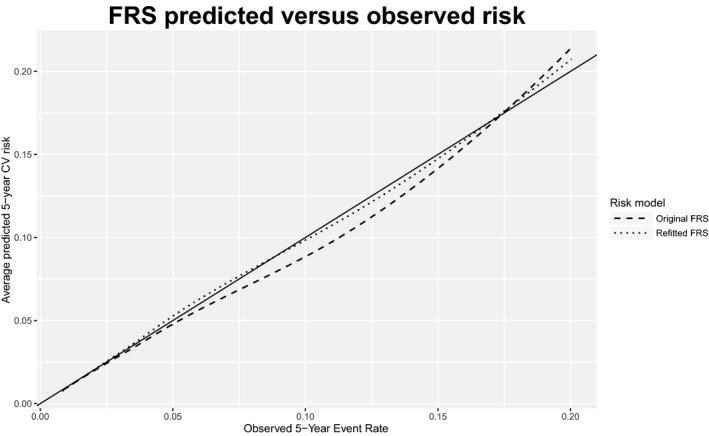
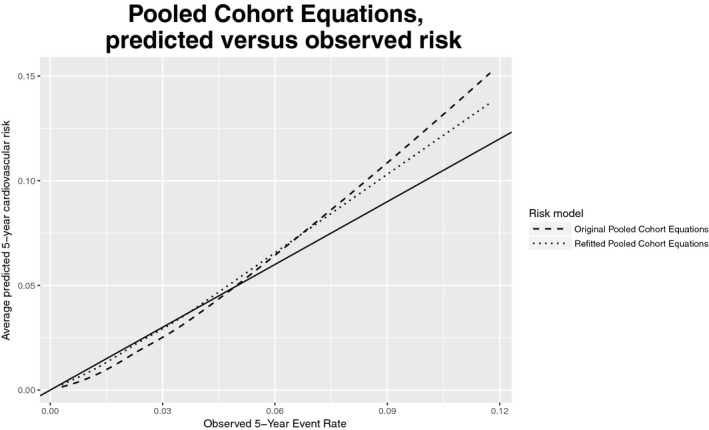
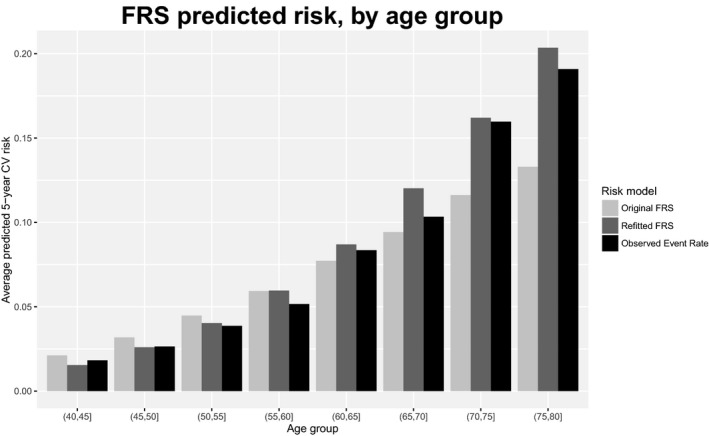
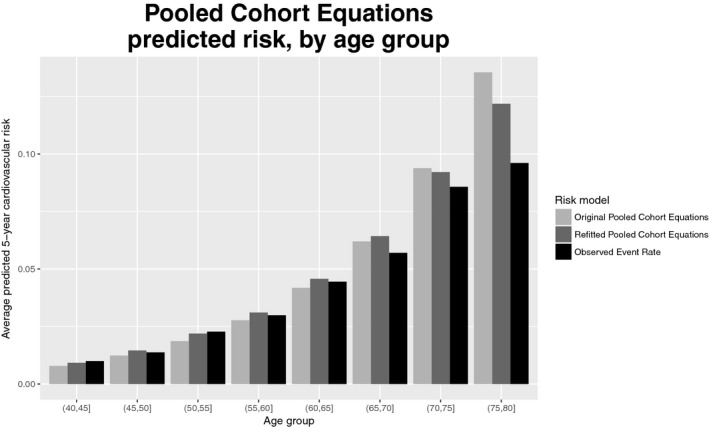
Methods and results: Data were extracted from the EHD of 84 116 adults aged 40 to 79 years who received care at a large healthcare delivery and insurance organization between 2001 and 2011. We assessed calibration and discrimination for 4 risk scores: published versions of FRS and PCE and versions obtained by refitting models using a subset of the available EHD. The published FRS was well calibrated (calibration statistic K=9.1, miscalibration ranging from 0% to 17% across risk groups), but the PCE displayed modest evidence of miscalibration (calibration statistic K=43.7, miscalibration from 9% to 31%). Discrimination was similar in both models (C-index=0.740 for FRS, 0.747 for PCE). Refitting the published models using EHD did not substantially improve calibration or discrimination.
Conclusions: We conclude that published cardiovascular risk models can be successfully applied to EHD to estimate cardiovascular risk; the FRS remains valid and is not obsolete; and model refitting does not meaningfully improve the accuracy of risk estimates.
Keywords: electronic health record data; risk prediction; risk score.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Implementing Cardiovascular Risk Prediction in Clinical Practice: The Future Is Now.J Am Heart Assoc. 2017 Apr 24;6(4):e006019. doi: 10.1161/JAHA.117.006019. J Am Heart Assoc. 2017. PMID: 28438743 Free PMC article. No abstract available.
References
-
- Stone NJ, Robinson J, Lichtenstein AH, Bairey Merz CN, Lloyd‐Jones DM, Blum CB, McBride P, Eckel RH, Schwartz JS, Goldberg AC, Shero ST, Gordon D, Smith SC, Levy D, Watson K, Wilson PWF. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:2889–2934. - PubMed
-
- Goff DC, Lloyd‐Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, Robinson J, Schwartz JS, Shero ST, Smith SC, Sorlie P, Stone NJ, Wilson PWF. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S49–S73. - PubMed
-
- D'Agostino RB, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117:743–753. - PubMed
-
- D'Agostino RB, Grundy S, Sullivan LM, Wilson P. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA. 2001;286:180–187. - PubMed
-
- Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med. 2007;356:2388–2398. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
