

Psychiatric associations of adult-onset focal dystonia phenotypes
- PMID: 28438790
- PMCID: PMC5659143
- DOI: 10.1136/jnnp-2016-315461
Psychiatric associations of adult-onset focal dystonia phenotypes
Abstract
Background: Depression and anxiety frequently accompany the motor manifestations of isolated adult-onset focal dystonias. Whether the body region affected when this type of dystonia first presents is associated with the severity of these neuropsychiatric symptoms is unknown.
Objectives: The aim of this study was to determine whether depression, anxiety and social anxiety vary by dystonia onset site and evaluate whether pain and dystonia severity account for any differences.
Methods: Patients with isolated focal dystonia evaluated within 5 years from symptom onset, enrolled in the Natural History Project of the Dystonia Coalition, were included in the analysis. Individual onset sites were grouped into five body regions: cervical, laryngeal, limb, lower cranial and upper cranial. Neuropsychiatric symptoms were rated using the Beck Depression Inventory, Hospital Anxiety and Depression Scale and Liebowitz Social Anxiety Scale. Pain was estimated using the 36-Item Short Form Survey.
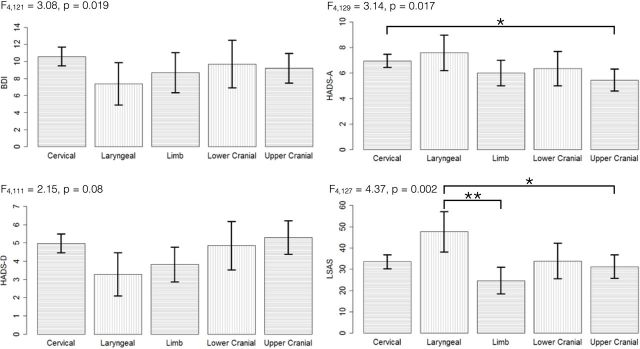
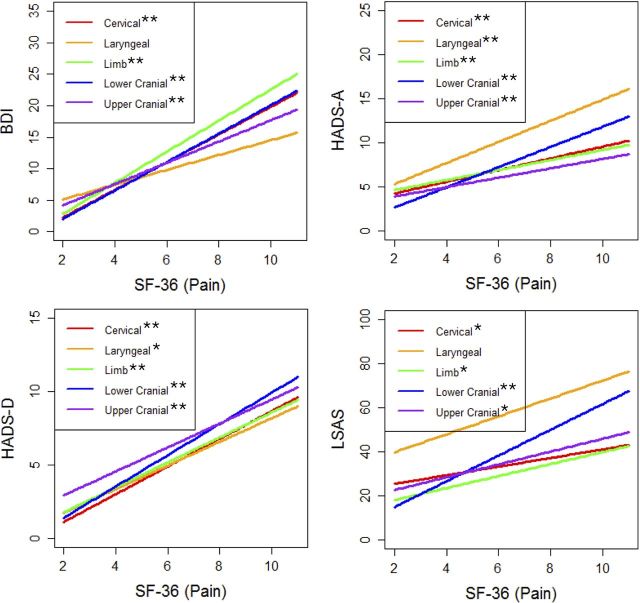
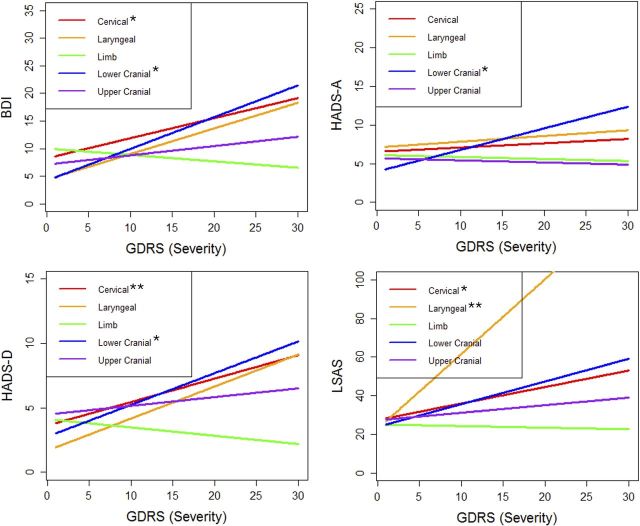
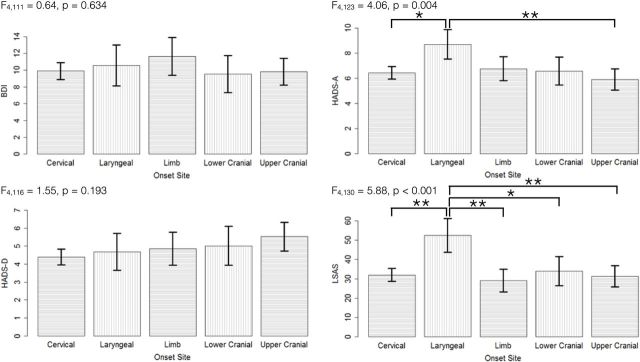
Results: Four hundred and seventy-eight subjects met our inclusion criteria. High levels of depression, anxiety and social anxiety occurred in all groups; however, the severity of anxiety and social anxiety symptoms varied by onset site group. The most pronounced differences were higher anxiety in cervical and laryngeal, lower anxiety in upper cranial and higher social anxiety in laryngeal. Increases in pain were associated with worse neuropsychiatric symptom scores within all groups. Higher anxiety and social anxiety in laryngeal and lower anxiety in upper cranial persisted after correcting for pain and dystonia severity.
Conclusion: Anxiety and social anxiety severity vary by onset site of focal dystonia, and this variation is not explained by differences in pain and dystonia severity.
Keywords: Isolated focal dystonia; anxiety; depression; pain.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Bressman SB. Dystonia genotypes, phenotypes, and classification. Adv Neurol 2004;94:101–7. - PubMed
-
- Defazio G. Epidemiology of Primary and Secondary Dystonia : Stacy MA, Handbook of Dystonia. New York, NY: Informa Healthcare USA, Inc, 2007:11–20.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous