

Prognostic Nomograms Stratify Survival of Patients with Hepatocellular Carcinoma Without Portal Vein Tumor Thrombosis After Curative Resection
- PMID: 28438885
- PMCID: PMC5423510
- DOI: 10.1634/theoncologist.2016-0231
Prognostic Nomograms Stratify Survival of Patients with Hepatocellular Carcinoma Without Portal Vein Tumor Thrombosis After Curative Resection
Abstract
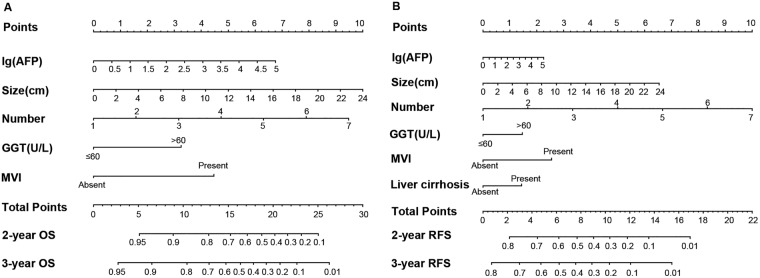
Background: The prognosis of patients with hepatocellular carcinoma (HCC) without portal vein tumor thrombosis (PVTT) after curative resection is at variance. We identified the risk factors of poor postoperative prognosis and consequently developed prognostic nomograms generating individual risk of death and recurrence for this subgroup of patients with HCC.
Methods: The risk factors were identified and nomograms were developed based on a retrospective study of 734 patients in the primary cohort who underwent curative resection for HCC from 2010 to 2012. The predictive accuracy and discriminative ability of the nomograms were determined by concordance index (C-index) and calibration curve and compared with traditional staging systems of HCC. The results were validated in an independent cohort of 349 patients operated at the same institution in 2007.
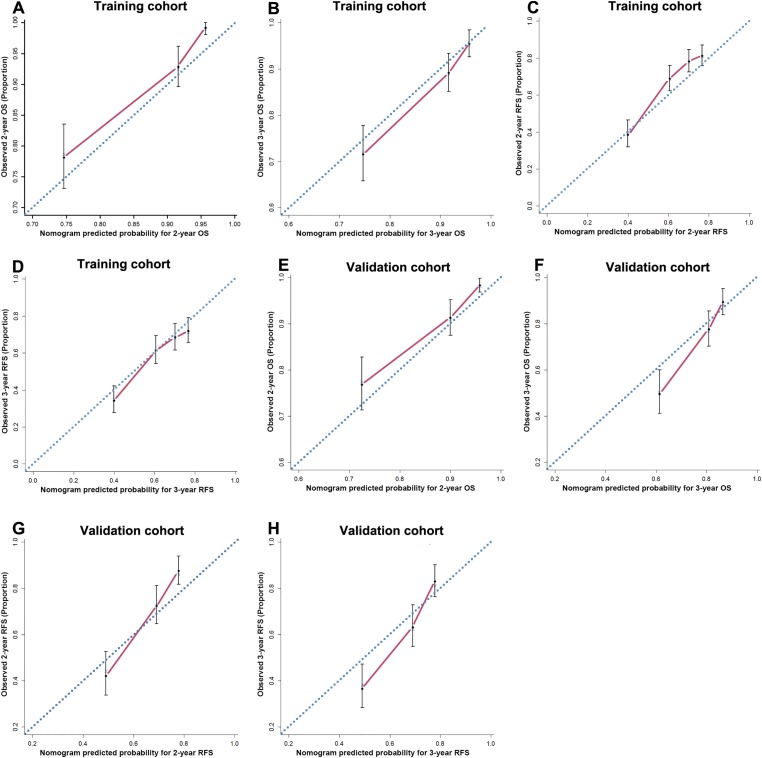
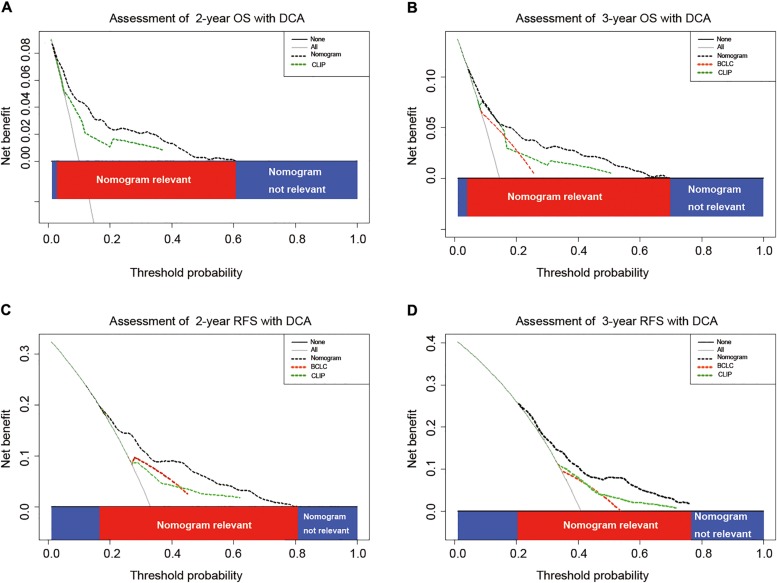
Results: All of the independent factors for survival in multivariate analysis in the primary cohort were selected into the nomograms. The calibration curve for probability of survival showed good agreement between prediction by nomograms and actual observation. The C-indices of the nomograms for predicting overall survival and recurrence-free survival were 0.755 (95% confidence interval [CI], 0.752-0.758) and 0.665 (95% CI, 0.662-0.668), respectively, which were statistically higher than the C-indices of other HCC prognostic models. The results were further confirmed in the validation cohort.
Conclusion: The proposed nomograms resulted in more accurate prognostic prediction for patients with HCC without PVTT after curative resection. The Oncologist 2017;22:561-569 IMPLICATIONS FOR PRACTICE: Hepatocellular carcinoma (HCC) poses a great therapeutic challenge due to the poor prognosis in patients underwent surgical resection. The portal vein tumor thrombosis (PVTT) as a robust risk factor for survival has been routinely integrated to staging systems. Nonetheless, the prognosis stratification for patients without PVTT was neglected to some extent. Herein, independent risk factors of OS and RFS in HCC patients without PVTT were reconfirmed. A predictive nomogram was constructed on these risk factors and was demonstrated to be a more accurate predictive model in HCC patients without PVTT, compared with the traditional staging systems.
摘要
背景. 业内对于无PVTT的HCC患者行根治性切除术后的预后仍有争议。我们已识别出这一HCC患者亚组术后预后不良的风险因素, 并据此开发了可生成各种死亡和复发风险的预后列线图。
方法. 对2010‐2012年间行根治性切除术治疗HCC的734例患者(主要队列)进行了一项回顾性研究, 在此基础之上识别风险因素并开发列线图。通过一致性指数(C指数)和校准曲线确定列线图的预测准确度和判别能力, 并与传统HCC分期系统进行比较。在一个独立队列, 即于2007年在同一机构接受手术的349例患者中验证所得结果。
结果. 将主要队列多变量分析中生存期的所有独立风险因素纳入列线图。在生存概率校准曲线中, 列线图预测值与实际观测值的吻合度较好。列线图预测总生存期和无复发生存期时的C指数分别为0.755[95%置信区间(CI):0.752‐0.758]和0.665(95% CI:0662‐0.668), 显著高于其他HCC预后模型的C指数。该结果在验证队列中得到了进一步确认。
结论. 本研究构建的列线图可以更准确地预测无PVTT的HCC患者行根治性切除术后的预后。The Oncologist 2017;22:561–569
对临床实践的提示:肝细胞癌(HCC)患者行切除手术后的预后较差, 从而给治疗带来了严峻挑战。门静脉癌栓(PVTT)是生存期的稳健风险因素之一, 已在常规实践中将其纳入分期系统。尽管如此, 我们仍在一定程度上忽视了无PVTT患者的预后分层。因此, 本研究在无PVTT的HCC患者中再次确认了总生存期(OS)和无复发生存期(RFS)的独立风险因素。针对上述风险因素构建了预测列线图, 结果证明在无PVTT的HCC患者中, 以该列线图作为预测模型时的准确度高于传统分期系统。
Keywords: Hepatocellular carcinoma; Nomogram; Portal vein tumor thrombosis; Prognosis; Resection.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
Similar articles
-
Postoperative adjuvant TACE-associated nomogram for predicting the prognosis of resectable Hepatocellular Carcinoma with portal vein Tumor Thrombus after Liver Resection.Int J Biol Sci. 2020 Oct 23;16(16):3210-3220. doi: 10.7150/ijbs.46896. eCollection 2020. Int J Biol Sci. 2020. PMID: 33162826 Free PMC article.
-
Novel Models Predict Postsurgical Recurrence and Overall Survival for Patients with Hepatitis B Virus-Related Solitary Hepatocellular Carcinoma ≤10 cm and Without Portal Venous Tumor Thrombus.Oncologist. 2020 Oct;25(10):e1552-e1561. doi: 10.1634/theoncologist.2019-0766. Epub 2020 Aug 6. Oncologist. 2020. PMID: 32663354 Free PMC article.
-
Nomogram predicting survival of hepatocellular carcinoma with portal vein tumour thrombus after curative resection.ANZ J Surg. 2019 Jan;89(1-2):E20-E25. doi: 10.1111/ans.14708. Epub 2018 Aug 17. ANZ J Surg. 2019. PMID: 30117625 Clinical Trial.
-
A systematic review comparing outcomes of surgical resection and non-surgical treatments for patients with hepatocellular carcinoma and portal vein tumor thrombus.HPB (Oxford). 2018 Dec;20(12):1119-1129. doi: 10.1016/j.hpb.2018.06.1804. Epub 2018 Jul 25. HPB (Oxford). 2018. PMID: 30056066
-
The strategies for treating primary hepatocellular carcinoma with portal vein tumor thrombus.Int J Surg. 2015 Aug;20:8-16. doi: 10.1016/j.ijsu.2015.05.009. Epub 2015 May 27. Int J Surg. 2015. PMID: 26026424 Review.
Cited by
-
Screening seven hub genes associated with prognosis and immune infiltration in glioblastoma.Front Genet. 2022 Aug 12;13:924802. doi: 10.3389/fgene.2022.924802. eCollection 2022. Front Genet. 2022. PMID: 36035134 Free PMC article.
-
Novel postoperative nomograms for predicting individual prognoses of hepatitis B-related hepatocellular carcinoma with cirrhosis.BMC Surg. 2022 Sep 13;22(1):339. doi: 10.1186/s12893-022-01789-4. BMC Surg. 2022. PMID: 36100893 Free PMC article. Clinical Trial.
-
High expression of Oct4 and Nanog predict poor prognosis in intrahepatic cholangiocarcinoma patients after curative resection.J Cancer. 2019 Jan 30;10(5):1313-1324. doi: 10.7150/jca.28349. eCollection 2019. J Cancer. 2019. PMID: 30854141 Free PMC article.
-
Novel Prognostic Nomograms for Hepatocellular Carcinoma Patients with Microvascular Invasion: Experience from a Single Center.Gut Liver. 2019 Nov 15;13(6):669-682. doi: 10.5009/gnl18489. Gut Liver. 2019. PMID: 30970430 Free PMC article.
-
Prognostic nomogram for hepatocellular carcinoma with radiofrequency ablation: a retrospective cohort study.BMC Cancer. 2021 Jun 29;21(1):751. doi: 10.1186/s12885-021-08505-0. BMC Cancer. 2021. PMID: 34187430 Free PMC article.
References
-
- Torre LA, Bray F, Siegel RL et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
