

Comparison of multiple non-invasive methods of measuring cardiac output during pregnancy reveals marked heterogeneity in the magnitude of cardiac output change between women
- PMID: 28438984
- PMCID: PMC5408281
- DOI: 10.14814/phy2.13223
Comparison of multiple non-invasive methods of measuring cardiac output during pregnancy reveals marked heterogeneity in the magnitude of cardiac output change between women
Abstract
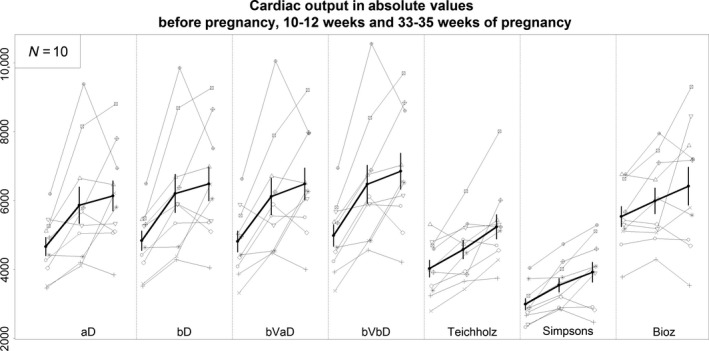
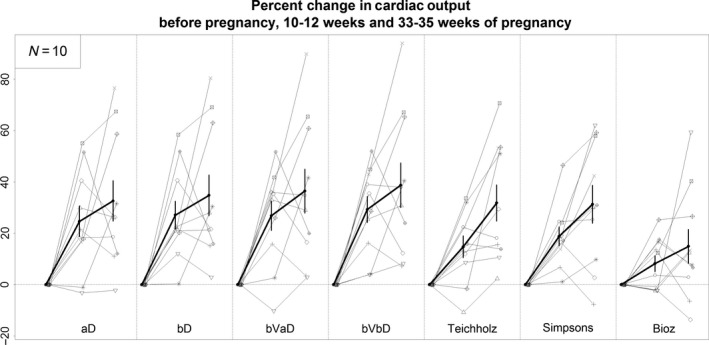
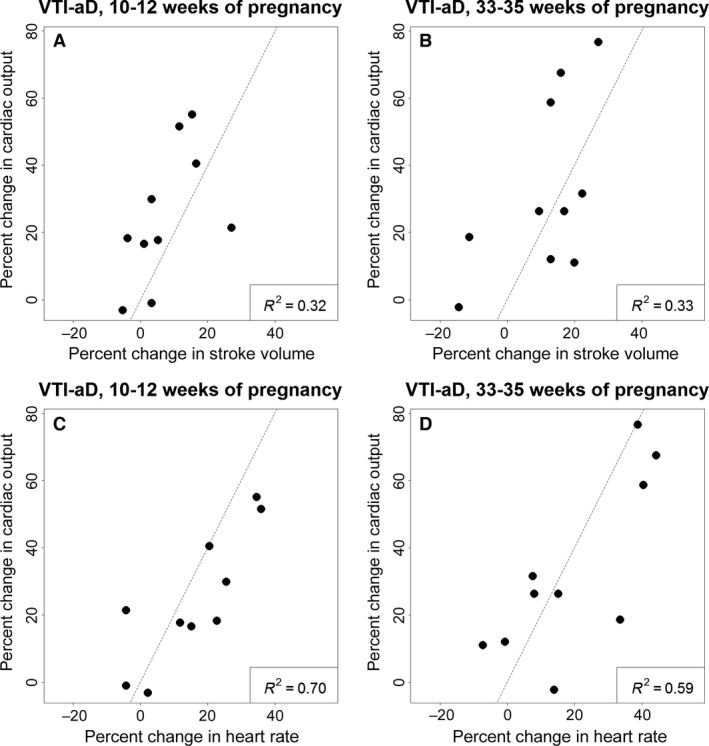
Various non-invasive methods are available to measure cardiac output (CO) during pregnancy. We compared serial measures of CO using various methods to determine which provided the least variability. Ten patients with spontaneous pregnancy had estimation of CO at baseline prior to becoming pregnant and at the end of the first and third trimesters. Echocardiographic data were used to estimate CO using the Teichholz method, Simpson's biplane method, and the Doppler determined velocity time integral (VTI) method. In addition, a Bioz Dx device was used to estimate CO by impedance cardiography. CO estimated with the VTI method had the lowest beat-to-beat variability. CO estimated with the VTI method was higher than CO estimated with the 2D-Teichholz method and Simpson's method. The percent change in CO during pregnancy was similar for all echo methods (VTI, Teichholz, and Simpson's biplane). Baseline CO determined with impedance cardiography was higher than CO determined with the VTI method. However, change in CO during pregnancy was significantly lower when measured with impedance cardiography. There was marked heterogeneity in the degree of rise in CO during the first trimester (-3 to 55%). The wide variation in the gestational rise in CO was unexpected, and at least in part secondary to variable increase in heart rate. We recommend the use of the Doppler determined VTI method for the estimation of CO in pregnancy.
Keywords: Cardiac Output; echocardiography; pregnancy.
© 2017 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of The Physiological Society and the American Physiological Society.
Figures
References
-
- Arora, G. , Morss A. M., et al. 2010. Difference in left ventricular ejection fraction using teichholz formula and volumetric methods by cmr: implications for patient stratification and selection of therapy. J. Cardiovasc. Magn. Reson. 12(Suppl1):P202.
-
- Boer, P. , Roos J. C., et al. 1979. Measurement of cardiac output by impedance cardiography under various conditions. Am. J. Physiol. 237:H491–H496. - PubMed
-
- Capeless, E. L. , and Clapp J. F.. 1989. Cardiovascular changes in early phase of pregnancy. Am. J. Obstet. Gynecol. 161(6 Pt 1):1449–1453. - PubMed
-
- Clark, S. L. , Cotton D. B., et al. 1991. Position change and central hemodynamic profile during normal third‐trimester pregnancy and post partum. Am. J. Obstet. Gynecol. 164:883–887. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
