

Lissencephaly: Expanded imaging and clinical classification
- PMID: 28440899
- PMCID: PMC5526446
- DOI: 10.1002/ajmg.a.38245
Lissencephaly: Expanded imaging and clinical classification
Abstract
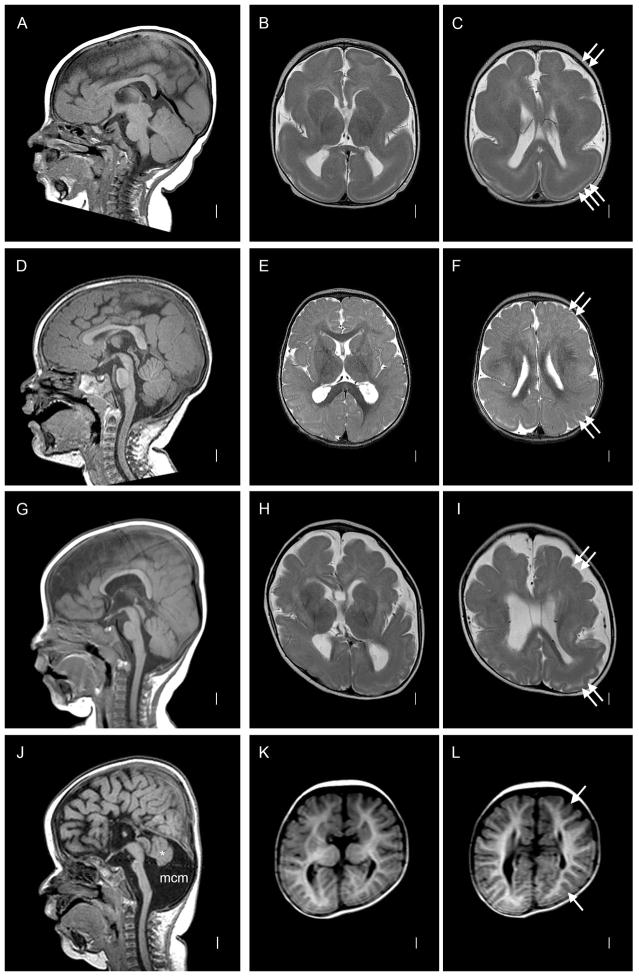
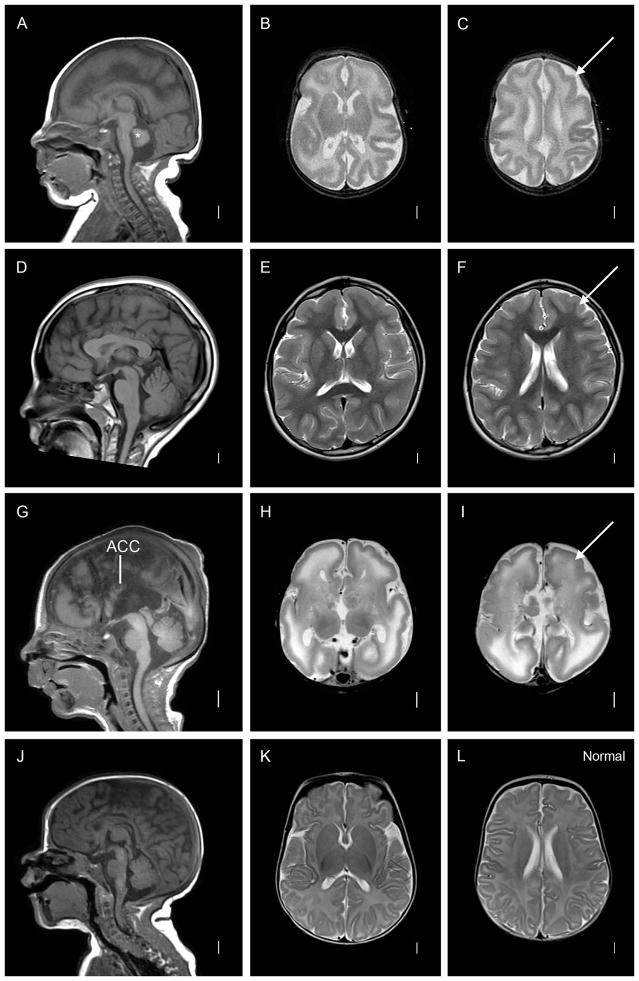
Lissencephaly ("smooth brain," LIS) is a malformation of cortical development associated with deficient neuronal migration and abnormal formation of cerebral convolutions or gyri. The LIS spectrum includes agyria, pachygyria, and subcortical band heterotopia. Our first classification of LIS and subcortical band heterotopia (SBH) was developed to distinguish between the first two genetic causes of LIS-LIS1 (PAFAH1B1) and DCX. However, progress in molecular genetics has led to identification of 19 LIS-associated genes, leaving the existing classification system insufficient to distinguish the increasingly diverse patterns of LIS. To address this challenge, we reviewed clinical, imaging and molecular data on 188 patients with LIS-SBH ascertained during the last 5 years, and reviewed selected archival data on another ∼1,400 patients. Using these data plus published reports, we constructed a new imaging based classification system with 21 recognizable patterns that reliably predict the most likely causative genes. These patterns do not correlate consistently with the clinical outcome, leading us to also develop a new scale useful for predicting clinical severity and outcome. Taken together, our work provides new tools that should prove useful for clinical management and genetic counselling of patients with LIS-SBH (imaging and severity based classifications), and guidance for prioritizing and interpreting genetic testing results (imaging based- classification).
Keywords: agyria; classification; lissencephaly; pachygyria; subcortical band heterotopia; tubulinopathy.
© 2017 Wiley Periodicals, Inc.
Figures



References
-
- Abdel-Salam GM, Abdel-Hamid MS, Hassan NA, Issa MY, Effat L, Ismail S, Aglan MS, Zaki MS. Further delineation of the clinical spectrum in RNU4ATAC related microcephalic osteodysplastic primordial dwarfism type I. Am J Med Genet. 2013;A161A:1875–1881. - PubMed
-
- Abdollahi MR, Morrison E, Sirey T, Molnar Z, Hayward BE, Carr IM, Springell K, Woods CG, Ahmed M, Hattingh L, Corry P, Pilz DT, Stoodley N, Crow Y, Taylor GR, Bonthron DT, Sheridan E. Mutation of the variant alpha-tubulin TUBA8 results in polymicrogyria with optic nerve hypoplasia. Am J Hum Genet. 2009;85:737–744. - PMC - PubMed
-
- Ashwal S, Michelson D, Plawner L, Dobyns WB Quality Standards Subcommittee of the American Academy of N, the Practice Committee of the Child Neurology S. Practice parameter: Evaluation of the child with microcephaly (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2009;73:887–897. - PMC - PubMed
-
- Bahi-Buisson N, Poirier K, Fourniol F, Saillour Y, Valence S, Lebrun N, Hully M, Bianco CF, Boddaert N, Elie C, Lascelles K, Souville I, Beldjord C, Chelly J. The wide spectrum of tubulinopathies: what are the key features for the diagnosis? Brain : a journal of neurology. 2014;137:1676–1700. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
