

Patient-Specific Classification of ICU Sedation Levels From Heart Rate Variability
- PMID: 28441231
- PMCID: PMC5474145
- DOI: 10.1097/CCM.0000000000002364
Patient-Specific Classification of ICU Sedation Levels From Heart Rate Variability
Abstract
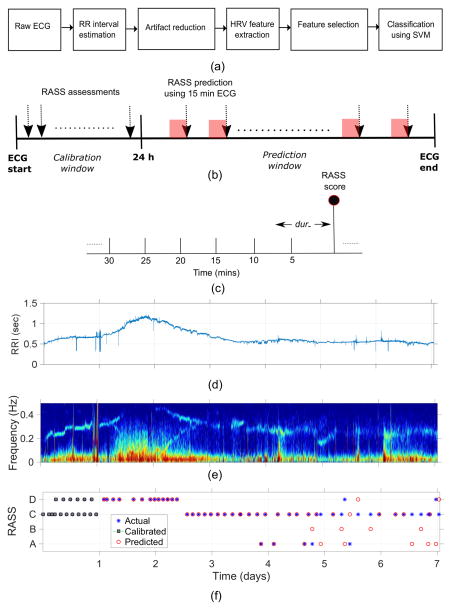
Objective: To develop a personalizable algorithm to discriminate between sedation levels in ICU patients based on heart rate variability.
Design: Multicenter, pilot study.
Setting: Several ICUs at Massachusetts General Hospital, Boston, MA.
Patients: We gathered 21,912 hours of routine electrocardiogram recordings from a heterogenous group of 70 adult ICU patients. All patients included in the study were mechanically ventilated and were receiving sedatives.
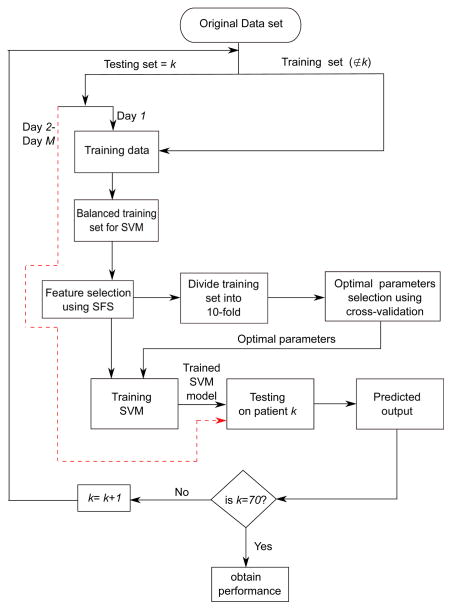
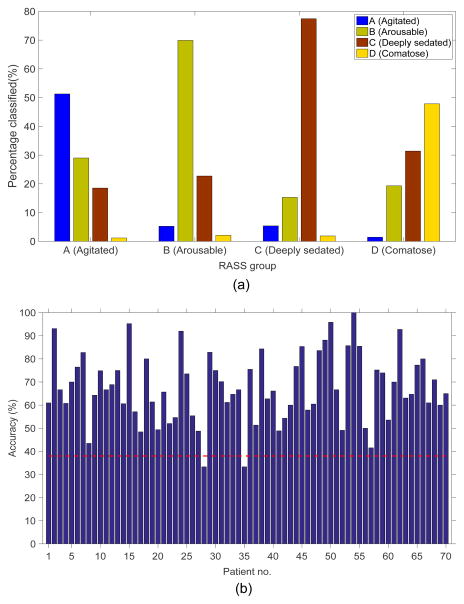
Measurements and main results: As "ground truth" for developing our method, we used Richmond Agitation Sedation Scale scores grouped into four levels denoted "comatose" (-5), "deeply sedated" (-4 to -3), "lightly sedated" (-2 to 0), and "agitated" (+1 to +4). We trained a support vector machine learning algorithm to calculate the probability of each sedation level from heart rate variability measures derived from the electrocardiogram. To estimate algorithm performance, we calculated leave-one-subject out cross-validated accuracy. The patient-independent version of the proposed system discriminated between the four sedation levels with an overall accuracy of 59%. Upon personalizing the system supplementing the training data with patient-specific calibration data, consisting of an individual's labeled heart rate variability epochs from the preceding 24 hours, accuracy improved to 67%. The personalized system discriminated between light- and deep-sedation states with an average accuracy of 75%.
Conclusions: With further refinement, the methodology reported herein could lead to a fully automated system for depth of sedation monitoring. By enabling monitoring to be continuous, such technology may help clinical staff to monitor sedation levels more effectively and to reduce complications related to over- and under sedation.
Figures
Comment in
-
Getting to Patients' Heads Through Their Hearts.Crit Care Med. 2017 Jul;45(7):1257-1258. doi: 10.1097/CCM.0000000000002422. Crit Care Med. 2017. PMID: 28622227 No abstract available.
References
-
- Pomeranz B, Macaulay RJ, Caudill MA, et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am J Physiol. 1985;248:H151–153. - PubMed
-
- Gehlbach BK, Kress JP. Sedation in the intensive care unit. Curr Opin Crit Care. 2002;8:290–298. - PubMed
-
- De Jonghe B, Cook D, Appere-De-Vecchi C, et al. Using and understanding sedation scoring systems: a systematic review. Intensive Care Med. 2000;26:275–285. - PubMed
-
- Jospin M, Caminal P, Jensen EW, et al. Detrended fluctuation analysis of EEG as a measure of depth of anesthesia. Biomed Eng IEEE Trans On. 2007;54:840–846. - PubMed
-
- Li X, Li D, Liang Z, et al. Analysis of depth of anesthesia with Hilbert–Huang spectral entropy. Clin Neurophysiol. 2008;119:2465–2475. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
