

Validation of an Administrative Definition of ICU Admission Using Revenue Center Codes
- PMID: 28441234
- PMCID: PMC5511059
- DOI: 10.1097/CCM.0000000000002374
Validation of an Administrative Definition of ICU Admission Using Revenue Center Codes
Abstract
Objectives: Describe the operating characteristics of a proposed set of revenue center codes to correctly identify ICU stays among hospitalized patients.
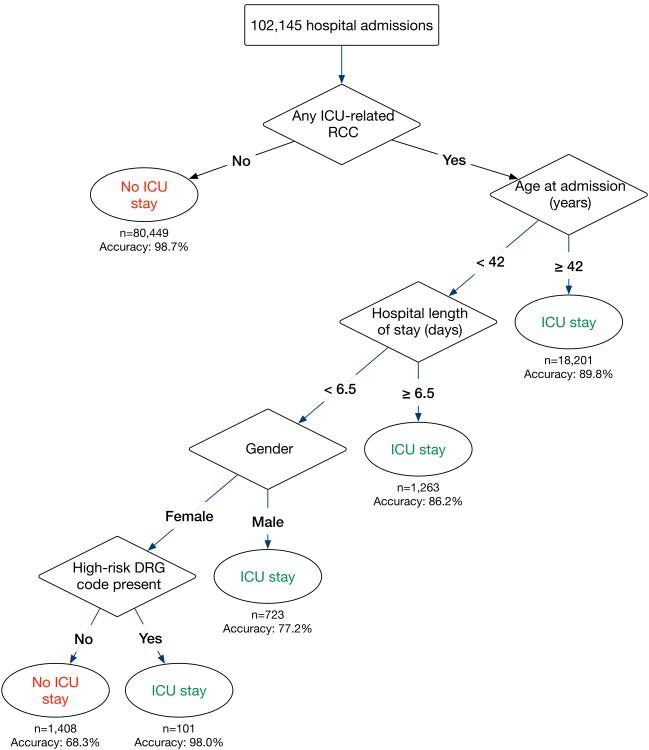
Design: Retrospective cohort study. We report the operating characteristics of all ICU-related revenue center codes for intensive and coronary care, excluding nursery, intermediate, and incremental care, to identify ICU stays. We use a classification and regression tree model to further refine identification of ICU stays using administrative data. The gold standard for classifying ICU admission was an electronic patient location tracking system.
Setting: The University of Pennsylvania Health System in Philadelphia, PA, United States.
Patients: All adult inpatient hospital admissions between July 1, 2013, and June 30, 2015.
Interventions: None.
Measurements and main results: Among 127,680 hospital admissions, the proposed combination of revenue center codes had 94.6% sensitivity (95% CI, 94.3-94.9%) and 96.1% specificity (95% CI, 96.0-96.3%) for correctly identifying hospital admissions with an ICU stay. The classification and regression tree algorithm had 92.3% sensitivity (95% CI, 91.6-93.1%) and 97.4% specificity (95% CI, 97.2-97.6%), with an overall improved accuracy (χ = 398; p < 0.001).
Conclusions: Use of the proposed combination of revenue center codes has excellent sensitivity and specificity for identifying true ICU admission. A classification and regression tree algorithm with additional administrative variables offers further improvements to accuracy.
Conflict of interest statement
Dr. Kohn has disclosed that she does not have any potential conflicts of interest.
Figures
References
-
- Barrett M, Smith M, Elixhauser A, et al. Utilization of intensive care services, 2011. Agency for Healthcare Research and Quality Statistical Brief. 2014;185:1–14. - PubMed
-
- Kersten A, Milbrandt E, Rahim M, et al. How big is critical care in the US? Crit Care Med. 2003;31:A8.
-
- Wunsch H, Angus DC, Harrison DA, et al. Variation in critical care services across North America and Western Europe. Crit Care Med. 2008;36:2787–2793. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
