

Sex discordance in asthma and wheeze prevalence in two longitudinal cohorts
- PMID: 28441402
- PMCID: PMC5404857
- DOI: 10.1371/journal.pone.0176293
Sex discordance in asthma and wheeze prevalence in two longitudinal cohorts
Abstract
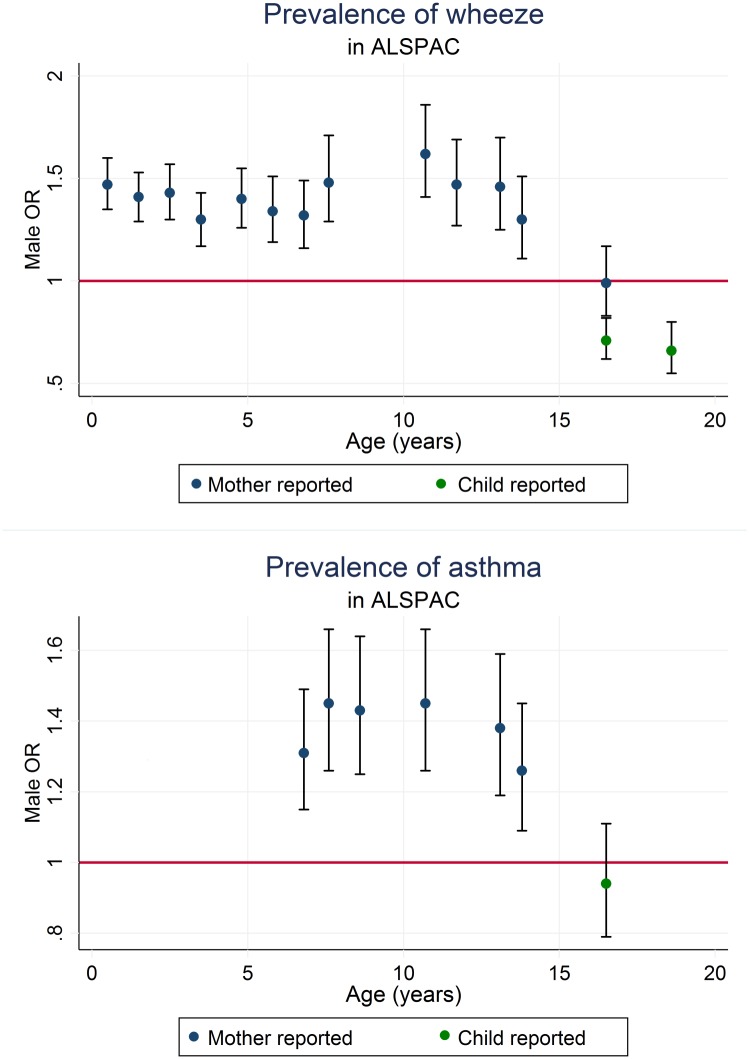
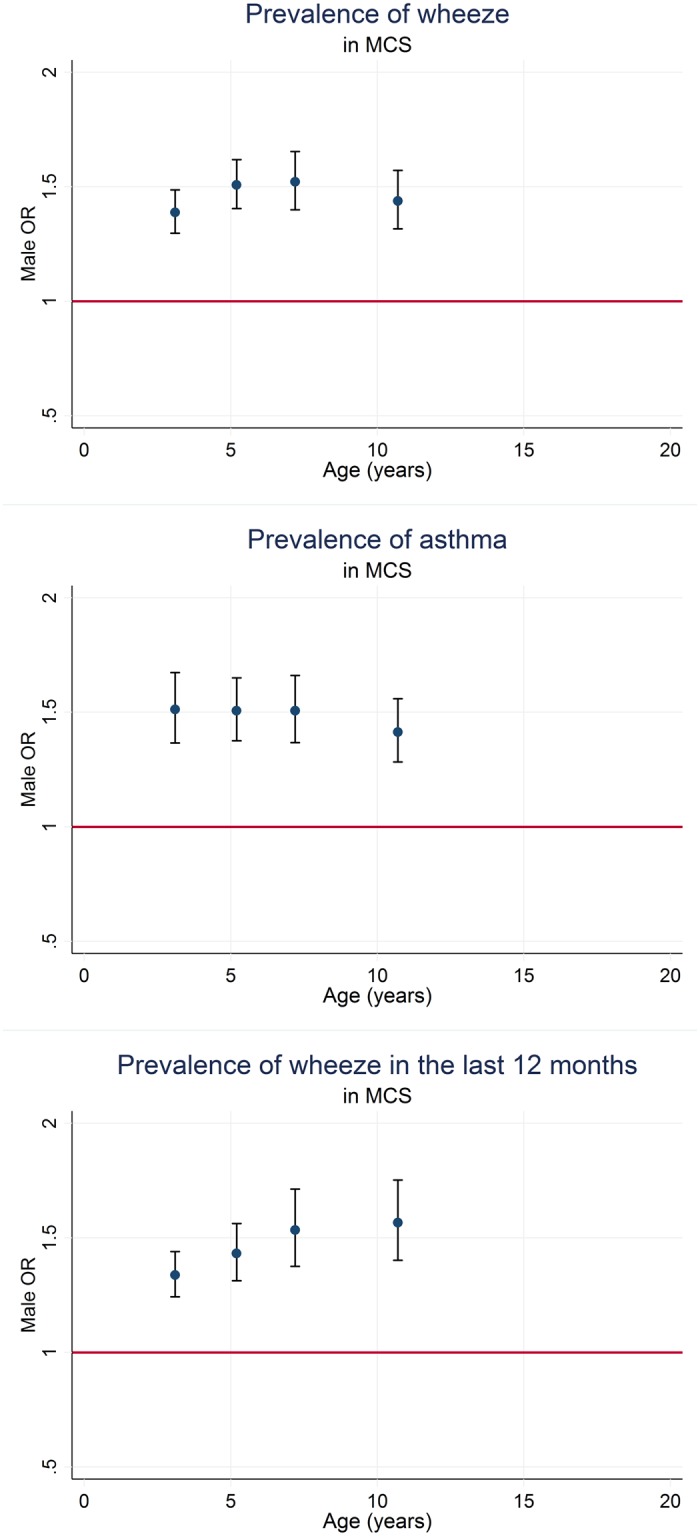
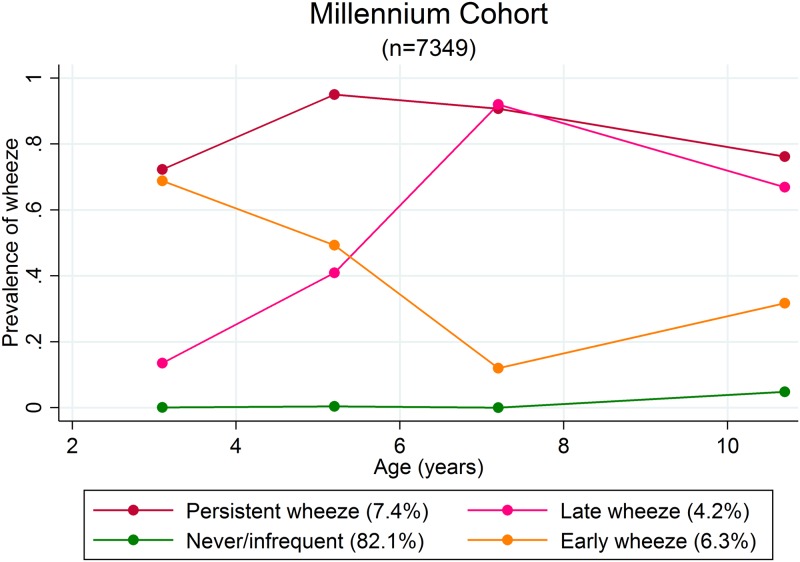
Sex discordance in asthma prevalence has been previously reported, with higher prevalence in males before puberty, and in females after puberty; the adolescent "switch". However, cross-sectional studies have suggested a narrowing of this discordance in recent decades. We used a combination of cross-sectional and longitudinal modelling to examine sex differences in asthma, wheeze and longitudinal wheezing phenotypes in two UK birth cohorts, the Avon Longitudinal Study of Parents and Children (ALSPAC; born 1991-92 with data from age 0-18 years) and the Millennium Cohort Study (MCS; born 2000-02 with data from age 3-10 years). We derived measures of asthma and wheeze from questionnaires completed by mothers and cohort children. Previously-derived ALSPAC wheezing phenotype models were applied to MCS. Males had a higher prevalence of asthma at 10.7 years in ALSPAC (OR 1.45 95%CI: 1.26, 1.66 n = 7778 for current asthma) and MCS (OR 1.42 95%CI: 1.29, 1.56 n = 6726 for asthma ever) compared to females, decreasing in ALSPAC after puberty (OR 0.94 95%CI: 0.79, 1.11 n = 5023 for current asthma at 16.5 years). In longitudinal models using restricted cubic splines, males had a clear excess for asthma in the last 12 months and wheeze in the last 12 months up until 16.5 years of age in ALSPAC. Males had an increased risk of all derived longitudinal wheezing phenotypes in MCS when compared to never wheeze and no evidence of being at lower risk of late wheeze when compared to early wheeze. By comparing data in two large, contemporary cohorts we have shown the persistence of sex discordance in childhood asthma, with no evidence that the sex discordance is narrowing in recent cohorts.
Conflict of interest statement
Figures

References
-
- Vink NM, Postma DS, Schouten JP, Rosmalen JGM, Boezen HM. Gender differences in asthma development and remission during transition through puberty: The TRacking Adolescents' Individual Lives Survey (TRAILS) study. Journal of Allergy and Clinical Immunology. 2010;126(3):498–504.e6. 10.1016/j.jaci.2010.06.018. - DOI - PubMed
-
- Worldwide variations in the prevalence of asthma symptoms: the International Study of Asthma and Allergies in Childhood (ISAAC). The European respiratory journal. 1998;12(2):315–35. Epub 1998/09/04. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
