

Evidence that promotion of male circumcision did not lead to sexual risk compensation in prioritized Sub-Saharan countries
- PMID: 28441458
- PMCID: PMC5404849
- DOI: 10.1371/journal.pone.0175928
Evidence that promotion of male circumcision did not lead to sexual risk compensation in prioritized Sub-Saharan countries
Abstract
Background: WHO and UNAIDS prioritized 14 eastern and southern African countries with high HIV and low male circumcision prevalence for a voluntary medical male circumcision (VMMC) scale-up in 2007. Because circumcision provides only partial protection against HIV infection to men, the issue of possible risk compensation in response to VMMC campaigns is of particular concern. In this study, we looked at population-level survey data from the countries prioritized by WHO for a VMMC scale-up. We compared the difference in sexual risk behaviours (SRB) between circumcised and uncircumcised men before and after the WHO's official VMMC promotion.
Materials and methods: Ten countries (Kenya, Lesotho, Malawi, Mozambique, Namibia, Rwanda, Tanzania, Uganda, Zambia and Zimbabwe) participating in the WHO's VMMC scale-up had available data from the Demographic and Health Surveys (DHS). We used cumulative-link mixed models to investigate interactions between survey period and circumcision status in predicting SRB, in order to evaluate whether the difference between the behavior of the two groups changed before and after the scale-up, while controlling for socio-demographic and knowledge-related covariates. The main responses were condom use at last sex and number of non-cohabiting sexual partners, both in the last 12 months.
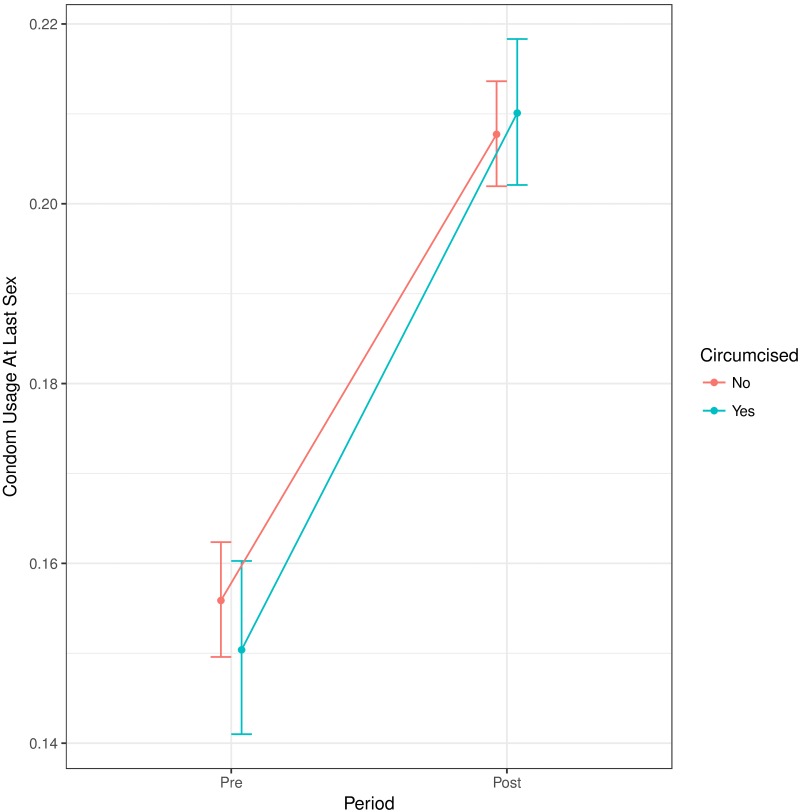
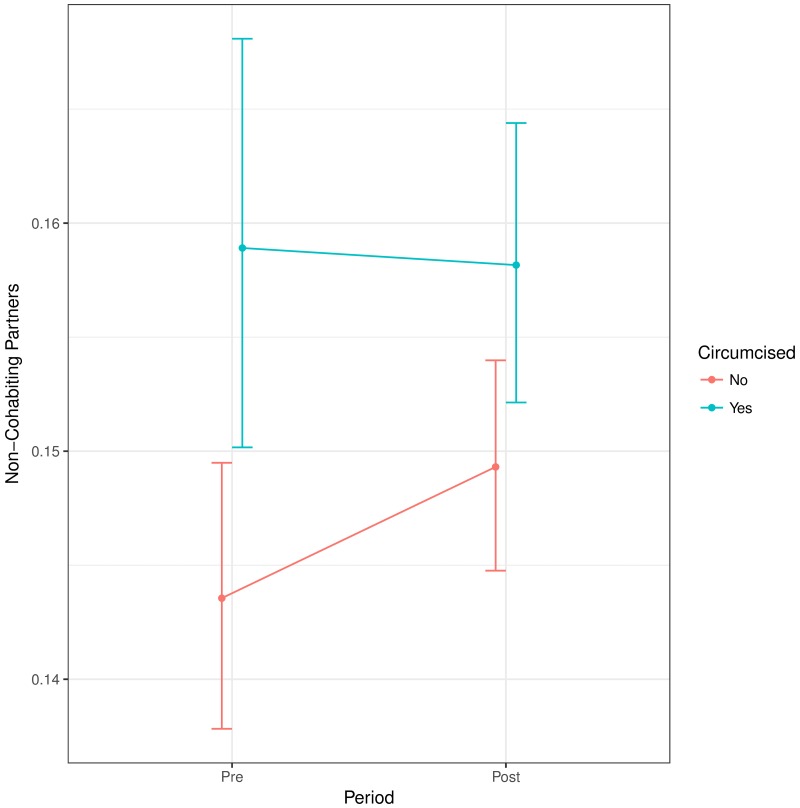
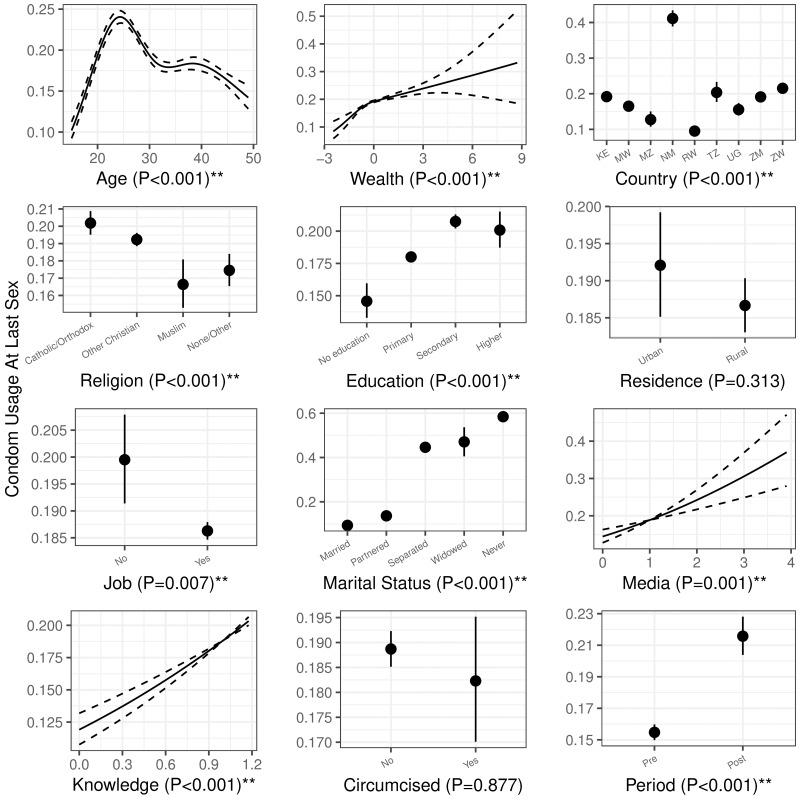
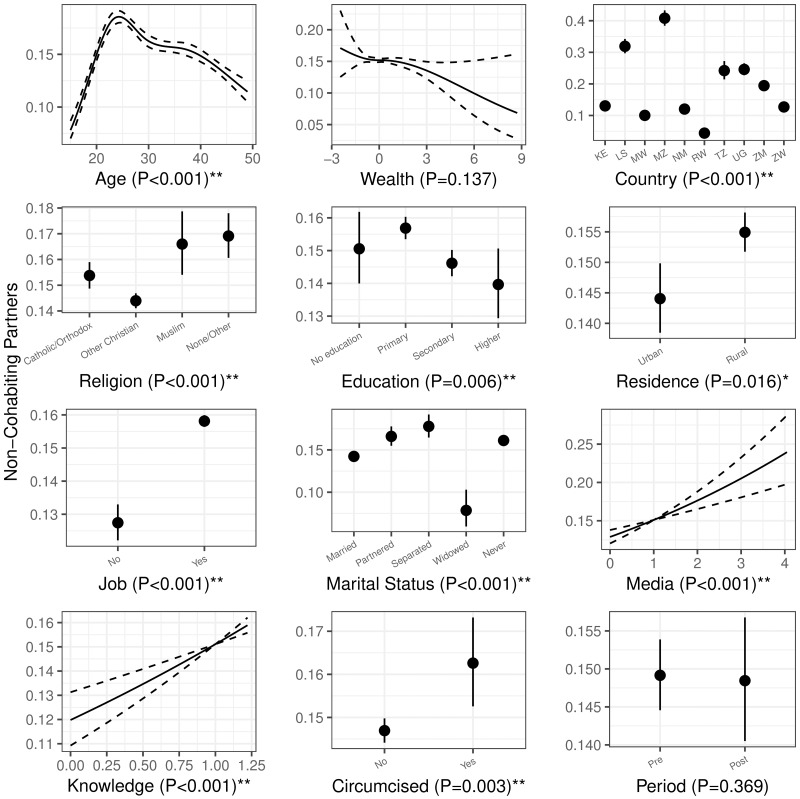
Results: There was little change in condom use by circumcised men relative to uncircumcised men from before the VMMC scale up to after the scale up. The relative odds ratio is 1.06 (95% CI, 0.95-1.18; interaction P = 0.310). Similarly, there was little change in the number of non-cohabiting partners in circumcised men (relative to uncircumcised men): the relative odds ratio of increasing the number of partners is 0.95 (95% CI, 0.86-1.05; interaction P = 0.319). Age, religion, education, job, marital status, media use and HIV knowledge also showed statistically significant association with the studied risk behaviours. We also found significant differences among countries, while controlling for covariates.
Conclusions: Overall, we find no evidence of sexual risk compensation in response to VMMC campaigns in countries prioritized by WHO. Changes in relative partner behaviour and the relative odds of condom use were small (and of uncertain sign). In fact, our estimates, though not significant, both suggest slightly less risky behavior. We conclude that sexual risk compensation in response to VMMC campaigns has not been a serious problem to date, but urge continued attention to local context, and to promulgating accurate messages about circumcision within and beyond the VMMC context.
Conflict of interest statement
Figures
Similar articles
-
Traditional Male Circumcision is Associated with Sexual Risk Behaviors in Sub-Saharan Countries Prioritized for Male Circumcision.AIDS Behav. 2020 Mar;24(3):951-959. doi: 10.1007/s10461-019-02473-0. AIDS Behav. 2020. PMID: 30955178
-
A comparison of sexual risk behaviours and HIV seroprevalence among circumcised and uncircumcised men before and after implementation of the safe male circumcision programme in Uganda.BMC Public Health. 2016 Jan 5;16:7. doi: 10.1186/s12889-015-2668-3. BMC Public Health. 2016. PMID: 26727935 Free PMC article.
-
Voluntary medical male circumcision and sexual practices among sexually active circumcised men in Mzuzu, Malawi: a cross-sectional study.BMC Public Health. 2020 Feb 11;20(1):211. doi: 10.1186/s12889-020-8309-5. BMC Public Health. 2020. PMID: 32046686 Free PMC article.
-
Economic compensation interventions to increase uptake of voluntary medical male circumcision for HIV prevention: A systematic review and meta-analysis.PLoS One. 2020 Jan 15;15(1):e0227623. doi: 10.1371/journal.pone.0227623. eCollection 2020. PLoS One. 2020. PMID: 31940422 Free PMC article.
-
Risk Compensation in Voluntary Medical Male Circumcision Programs.Curr HIV/AIDS Rep. 2022 Dec;19(6):516-521. doi: 10.1007/s11904-022-00635-9. Epub 2022 Nov 9. Curr HIV/AIDS Rep. 2022. PMID: 36350470 Review.
Cited by
-
Females' Peer Influence and Support for Adolescent Males Receiving Voluntary Medical Male Circumcision Services.Clin Infect Dis. 2018 Apr 3;66(suppl_3):S183-S188. doi: 10.1093/cid/cix1057. Clin Infect Dis. 2018. PMID: 29617773 Free PMC article.
-
Ethical implications of economic compensation for voluntary medical male circumcision for HIV prevention and epidemic control.PLOS Glob Public Health. 2022 Dec 16;2(12):e0001361. doi: 10.1371/journal.pgph.0001361. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962919 Free PMC article. Review.
-
A review of public health, social and ethical implications of voluntary medical male circumcision programs for HIV prevention in sub-Saharan Africa.Int J Impot Res. 2023 May;35(3):269-278. doi: 10.1038/s41443-021-00484-x. Epub 2021 Oct 26. Int J Impot Res. 2023. PMID: 34702986 Free PMC article. Review.
-
Widespread changes in sexual behaviour in eastern and southern Africa: Challenges to achieving global HIV targets? Longitudinal analyses of nationally representative surveys.J Int AIDS Soc. 2019 Jun;22(6):e25329. doi: 10.1002/jia2.25329. J Int AIDS Soc. 2019. PMID: 31225953 Free PMC article.
-
Service delivery interventions to increase uptake of voluntary medical male circumcision for HIV prevention: A systematic review.PLoS One. 2020 Jan 13;15(1):e0227755. doi: 10.1371/journal.pone.0227755. eCollection 2020. PLoS One. 2020. PMID: 31929587 Free PMC article.
References
-
- Alcena V. AIDS in Third world countries. New York State Journal of Medicine. 1986;86:44. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
