

Cannabis use is associated with reduced prevalence of non-alcoholic fatty liver disease: A cross-sectional study
- PMID: 28441459
- PMCID: PMC5404771
- DOI: 10.1371/journal.pone.0176416
Cannabis use is associated with reduced prevalence of non-alcoholic fatty liver disease: A cross-sectional study
Abstract
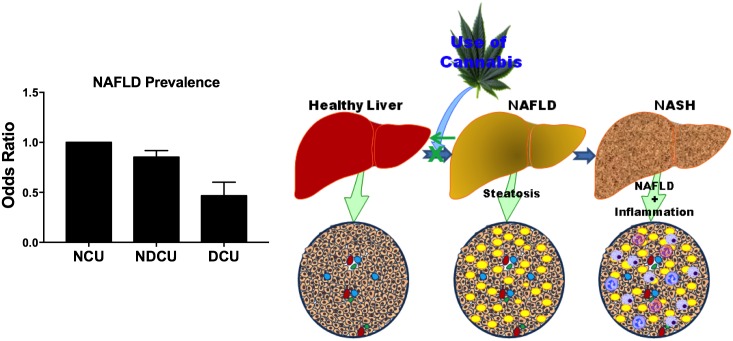
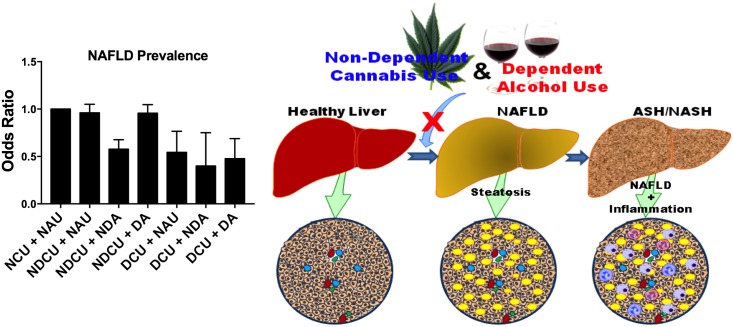
Cannabis use is associated with reduced prevalence of obesity and diabetes mellitus (DM) in humans and mouse disease models. Obesity and DM are a well-established independent risk factor for non-alcoholic fatty liver disease (NAFLD), the most prevalent liver disease globally. The effects of cannabis use on NAFLD prevalence in humans remains ill-defined. Our objective is to determine the relationship between cannabis use and the prevalence of NAFLD in humans. We conducted a population-based case-control study of 5,950,391 patients using the 2014 Healthcare Cost and Utilization Project (HCUP), Nationwide Inpatient Survey (NIS) discharge records of patients 18 years and older. After identifying patients with NAFLD (1% of all patients), we next identified three exposure groups: non-cannabis users (98.04%), non-dependent cannabis users (1.74%), and dependent cannabis users (0.22%). We adjusted for potential demographics and patient related confounders and used multivariate logistic regression (SAS 9.4) to determine the odds of developing NAFLD with respects to cannabis use. Our findings revealed that cannabis users (dependent and non-dependent) showed significantly lower NAFLD prevalence compared to non-users (AOR: 0.82[0.76-0.88]; p<0.0001). The prevalence of NAFLD was 15% lower in non-dependent users (AOR: 0.85[0.79-0.92]; p<0.0001) and 52% lower in dependent users (AOR: 0.49[0.36-0.65]; p<0.0001). Among cannabis users, dependent patients had 43% significantly lower prevalence of NAFLD compared to non-dependent patients (AOR: 0.57[0.42-0.77]; p<0.0001). Our observations suggest that cannabis use is associated with lower prevalence of NAFLD in patients. These novel findings suggest additional molecular mechanistic studies to explore the potential role of cannabis use in NAFLD development.
Conflict of interest statement
Figures
Similar articles
-
Cannabis use is associated with reduced prevalence of progressive stages of alcoholic liver disease.Liver Int. 2018 Aug;38(8):1475-1486. doi: 10.1111/liv.13696. Epub 2018 Feb 10. Liver Int. 2018. PMID: 29341392
-
Effects of Statin Use on the Development and Progression of Nonalcoholic Fatty Liver Disease: A Nationwide Nested Case-Control Study.Am J Gastroenterol. 2021 Jan 1;116(1):116-124. doi: 10.14309/ajg.0000000000000845. Am J Gastroenterol. 2021. PMID: 33027082
-
Prevalence of non-alcoholic fatty liver disease in patients with diabetes mellitus, hyperlipidemia, obesity and polycystic ovary syndrome: A cross-sectional study in north of Iran.Diabetes Metab Syndr. 2019 Mar-Apr;13(2):1591-1596. doi: 10.1016/j.dsx.2019.03.009. Epub 2019 Mar 8. Diabetes Metab Syndr. 2019. PMID: 31336526
-
Antiplatelet therapy associated with lower prevalence of advanced liver fibrosis in non-alcoholic fatty liver disease: A systematic review and meta-analysis.Indian J Gastroenterol. 2022 Apr;41(2):119-126. doi: 10.1007/s12664-021-01230-3. Epub 2022 Mar 22. Indian J Gastroenterol. 2022. PMID: 35318571
-
Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis.Lancet Gastroenterol Hepatol. 2020 Aug;5(8):739-752. doi: 10.1016/S2468-1253(20)30077-7. Epub 2020 May 12. Lancet Gastroenterol Hepatol. 2020. PMID: 32413340
Cited by
-
Canadian Association of Gastroenterology Position Statement: Use of Cannabis in Gastroenterological and Hepatic Disorders.J Can Assoc Gastroenterol. 2019 Apr;2(1):37-43. doi: 10.1093/jcag/gwy064. Epub 2018 Nov 8. J Can Assoc Gastroenterol. 2019. PMID: 31294362 Free PMC article. No abstract available.
-
Impacts of medical and non-medical cannabis on the health of older adults: Findings from a scoping review of the literature.PLoS One. 2023 Feb 17;18(2):e0281826. doi: 10.1371/journal.pone.0281826. eCollection 2023. PLoS One. 2023. PMID: 36800328 Free PMC article.
-
The Effect of Oil-Based Cannabis Extracts on Metabolic Parameters and Microbiota Composition of Mice Fed a Standard and a High-Fat Diet.Int J Mol Sci. 2024 Jan 16;25(2):1073. doi: 10.3390/ijms25021073. Int J Mol Sci. 2024. PMID: 38256146 Free PMC article.
-
Reduced Incidence and Better Liver Disease Outcomes among Chronic HCV Infected Patients Who Consume Cannabis.Can J Gastroenterol Hepatol. 2018 Sep 23;2018:9430953. doi: 10.1155/2018/9430953. eCollection 2018. Can J Gastroenterol Hepatol. 2018. PMID: 30345261 Free PMC article.
-
Marijuana is not associated with progression of hepatic fibrosis in liver disease: a systematic review and meta-analysis.Eur J Gastroenterol Hepatol. 2019 Feb;31(2):149-156. doi: 10.1097/MEG.0000000000001263. Eur J Gastroenterol Hepatol. 2019. PMID: 30234644 Free PMC article.
References
-
- United Nations Office on Drugs and Crime. World drug report 2012. [Internet]. New York: United Nations; 2012. http://search.ebscohost.com/login.aspx?direct=true&scope=site&db=nlebk&d...
-
- Substance Abuse and Mental Health Services Administration. Results from the 2014 National Survey on Drug Use and Health: National Findings. HHS Publication No. (SMA) 14–4863. Center for Behavioral Health Statistics and Quality, Rockville, MD:.;
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
