

Effects of unconditional cash transfers on the outcome of treatment for severe acute malnutrition (SAM): a cluster-randomised trial in the Democratic Republic of the Congo
- PMID: 28441944
- PMCID: PMC5405483
- DOI: 10.1186/s12916-017-0848-y
Effects of unconditional cash transfers on the outcome of treatment for severe acute malnutrition (SAM): a cluster-randomised trial in the Democratic Republic of the Congo
Abstract
Background: Cash transfer programs (CTPs) aim to strengthen financial security for vulnerable households. This potentially enables improvements in diet, hygiene, health service access and investment in food production or income generation. The effect of CTPs on the outcome of children already severely malnourished is not well delineated. The objective of this study was to test whether CTPs will improve the outcome of children treated for severe acute malnutrition (SAM) in the Democratic Republic of the Congo over 6 months.
Methods: We conducted a cluster-randomised controlled trial in children with uncomplicated SAM who received treatment according to the national protocol and counselling with or without a cash supplement of US$40 monthly for 6 months. Analyses were by intention to treat.
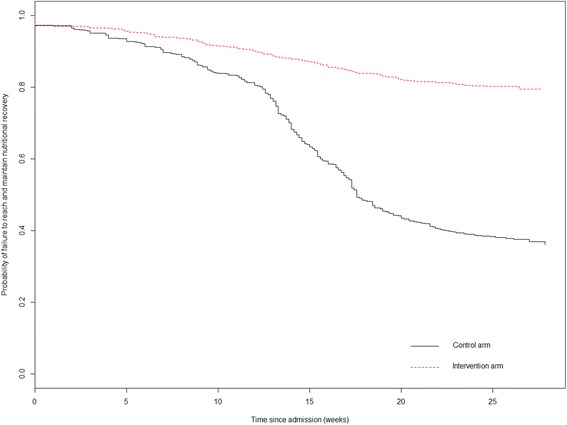
Results: The hazard ratio of reaching full recovery from SAM was 35% higher in the intervention group than the control group (adjusted hazard ratio, 1.35, 95% confidence interval (CI) = 1.10 to 1.69, P = 0.007). The adjusted hazard ratios in the intervention group for relapse to moderate acute malnutrition (MAM) and SAM were 0.21 (95% CI = 0.11 to 0.41, P = 0.001) and 0.30 (95% CI = 0.16 to 0.58, P = 0.001) respectively. Non-response and defaulting were lower when the households received cash. All the nutritional outcomes in the intervention group were significantly better than those in the control group. After 6 months, 80% of cash-intervened children had re-gained their mid-upper arm circumference measurements and weight-for-height/length Z-scores and showed evidence of catch-up. Less than 40% of the control group had a fully successful outcome, with many deteriorating after discharge. There was a significant increase in diet diversity and food consumption scores for both groups from baseline; the increase was significantly greater in the intervention group than the control group.
Conclusions: CTPs can increase recovery from SAM and decrease default, non-response and relapse rates during and following treatment. Household developmental support is critical in food insecure areas to maximise the efficiency of SAM treatment programs.
Trial registration: ClinicalTrials.gov, NCT02460848 . Registered on 27 May 2015.
Keywords: CMAM; Cash transfer; Cluster-randomised trial; Community-based management of acute malnutrition; Democratic Republic of the Congo; Malnutrition; Severe acute malnutrition.
Figures

References
-
- World Health Organization, World Food Programme, United Nations System Standing Committee on Nutrition, United Nations Children's Fund . Community-based management of severe acute malnutrition. A joint statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children's Fund. Geneva: World Health Organization; 2007.
-
- World Health Organization, United Nations Children's Fund . WHO child growth standards and the identification of severe acute malnutrition in infants and children. A joint statement by the World Health Organization and the United Nations Children's Fund. Geneva: World Health Organization; 2009. - PubMed
-
- World Health Organization . Guideline update: technical aspects of the management of severe acute malnutrition in infants and children. Geneva: World Health Organization; 2013. - PubMed
-
- Sen A. Poverty and famines: an essay on entitlement and deprivation. Oxford: Oxford University Press; 1981.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
