

In-hospital airway management training for non-anesthesiologist EMS physicians: a descriptive quality control study
- PMID: 28441963
- PMCID: PMC5405543
- DOI: 10.1186/s13049-017-0386-9
In-hospital airway management training for non-anesthesiologist EMS physicians: a descriptive quality control study
Abstract
Background: Pre-hospital airway management is a major challenge for emergency medical service (EMS) personnel. Despite convincing evidence that the rescuer's qualifications determine efficacy of tracheal intubation, in-hospital airway management training is not mandatory in Austria, and often neglected. Thus we sought to prove that airway management competence of EMS physicians can be established and maintained by a tailored training program.
Methods: In this descriptive quality control study we retrospectively evaluated all in- and pre-hospital airway cases managed by EMS physicians who underwent a structured in-hospital training program in anesthesia at General Hospital Wiener Neustadt. Data was obtained from electronic anesthesia and EMS documentation systems.
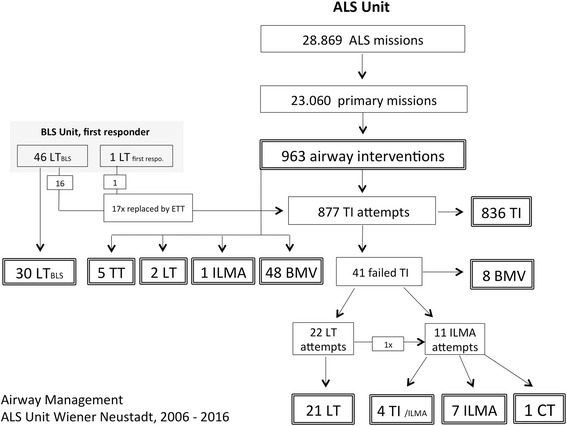
Results: From 2006 to 2016, 32 EMS physicians with 3-year post-graduate education, but without any prior experience in anesthesia were trained. Airway management proficiency was imparted in three steps: initial training, followed by an ongoing practice schedule in the operating room (OR). Median and interquartile range of number of in-hospital tracheal intubations (TIs) vs. use of supra-glottic airway devices (SGA) were 33.5 (27.5-42.5) vs. 19.0 (15.0-27.0) during initial training; 62.0 (41.8-86.5) vs. 33.5 (18.0-54.5) during the first, and 64.0 (34.5-93.8) vs. 27 (12.5-56.0) during the second year. Pre-hospitaly, every physician performed 9.0 (5.0-14.8) TIs vs. 0.0 (0.0-0.0) SGA cases during the first, and 9.0 (7.0-13.8) TIs vs. 0.0 (0.0-0.3) SGA during the second year. Use of an SGA was mandatory when TI failed after the second attempt, thus accounting for a total of 33 cases. In 8 cases, both TI and SGA failed, but bag mask ventilation was successfully performed. No critical events related to airway management were noted and overall success rate for TI with a max of 2 attempts was 95.3%.
Discussion: Number of TIs per EMS physician is low in the pre-hospital setting. A training concept that assures an additional 60+ TIs per year appears to minimize failure rates. Thus, a fixed amount of working days in anesthesia seems crucial to maintain proficiency. CONCLUSIONS: In-hospital training programs are mandatory for non-anesthetist EMS physicians to gain competence in airway management and emergency anesthesia.Our results might be helpful when discussing the need for regulation and financing with the authorities.
Keywords: Airway management; Difficult airway algorithm; Emergency anesthesia; Emergency physician; Quality control study; Tracheal intubation; Training.
Figures
References
-
- European Case Law Identifier (ECLI) ECLI:AT: OGH0002:2016:0090OB00076.15I.0225.000
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
