

Treatment-limiting decisions in patients with severe traumatic brain injury in a Norwegian regional trauma center
- PMID: 28441973
- PMCID: PMC5405474
- DOI: 10.1186/s13049-017-0385-x
Treatment-limiting decisions in patients with severe traumatic brain injury in a Norwegian regional trauma center
Abstract
Background: Treatment-limiting decisions (TLD) for severe traumatic brain injury (sTBI) have been sparsely studied. This study determine prevalence, main reason for, categories and timing of TLDs in a Norwegian regional trauma setting.
Methods: A retrospective study of a 2-year cohort of 579 sTBI patients admitted to Oslo University Hospital (OUH). Prospectively collected data in the OUH Trauma Registry were combined with retrospective data from a chart review regarding TLDs.
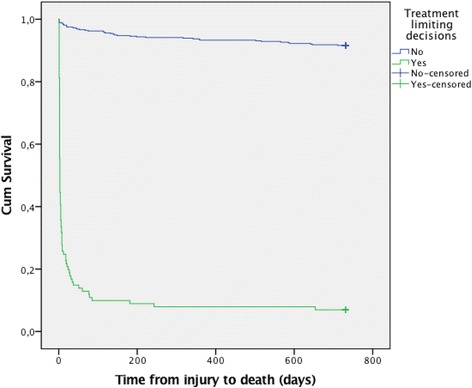
Results: TLDs were documented for 101/579 sTBI patients (17%). The situation was evaluated as futile in 59 cases and as potentially inappropriate in 42 cases. The three most frequent types of TLDs were withholding of neurosurgery, do not resuscitate orders and withdrawing of organ support. In 70% of cases, the first TLD was made within 2 days after injury, while in 14%, the first TLD was made later than day 7. Twenty percent (20/101) of the first TLDs were later adjusted, revoked in 4 patients and broadening of TLDs in 16 patients. The median time from the decision to death was 2 days (range 1-652). TLDs were documented in 93% of in-hospital death cases (n = 79). In-hospital deaths occurred in 73% of TLD group cases and 1% of non-TLD group cases. Family interaction and multi-team discussions were documented in >88% of cases, but no advanced directives were found, and notifications of patients' preferences were found in only 7% of cases.
Discussion: Clinicians should consider limiting treatment if continued treatment is not in the patients best interest. A range of different types of TLDs were applied for patients after sTBI in the trauma hospital setting.
Conclusion: TLDs were found in 17% of sTBI patients. Value considerations behind TLDs in this care context need to be further explored.
Keywords: Decision-making; Futility; Potentially inappropriate treatment; Traumatic brain injury; Withholding treatment.
Figures
References
-
- Norwegian Directorate of Health . National guideline: Decision-making processes in the limitation of life-prolonging treatment. Oslo, Norway: Norwegian Directorate of Health; 2013.
-
- Jennett B. Severe head injuries: ethical aspects of management. Br J Hosp Med. 1992;47(5):354–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
