

Comparing airways clearance techniques in chronic obstructive pulmonary disease and bronchiectasis: positive expiratory pressure or temporary positive expiratory pressure? A retrospective study
- PMID: 28442070
- PMCID: PMC5537431
- DOI: 10.1016/j.bjpt.2016.12.001
Comparing airways clearance techniques in chronic obstructive pulmonary disease and bronchiectasis: positive expiratory pressure or temporary positive expiratory pressure? A retrospective study
Abstract
Background: Airway clearance techniques include positive expiratory pressure, commonly used in our clinical practice, and a recently introduced temporary positive expiratory pressure device called UNIKO®. It is unclear which one provides the best benefit to patients.
Objectives: The aim of this observational 4-year study was to retrospectively compare the efficacy of and specific indications for temporary positive expiratory pressure compared to positive expiratory pressure in a standard rehabilitation program.
Method: We retrospectively collected data from 162 subjects (107 males, mean age 70±9 years, 97 with primary diagnosis of chronic obstructive pulmonary disease, 65 with bronchiectasis), 51 treated with temporary positive expiratory pressure and 111 with positive expiratory pressure.
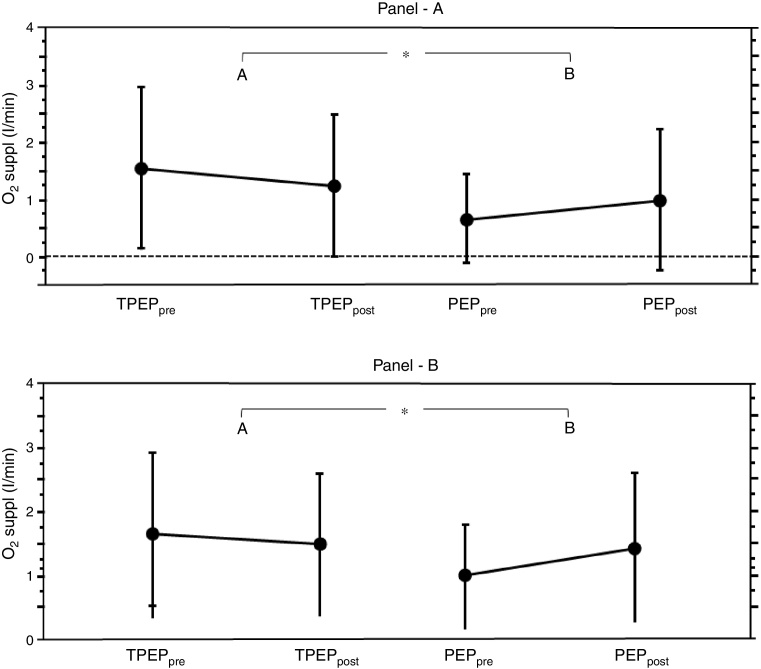
Results: Subjects showed significant improvement in ratio of partial pressure arterial oxygen and fraction of inspired oxygen (p<0.001), forced vital capacity, forced expiratory volume in one second, peak expiratory flow, arterial oxygen saturation, and partial pressure arterial oxygen with no significant difference between positive expiratory pressure and temporary positive expiratory pressure groups apart from forced expiratory flow, which increased only in the positive expiratory pressure group. Evaluating specific subgroups, temporary positive expiratory pressure was more effective than positive expiratory pressure in improving gas transfer in subjects with emphysema and in those on oxygen therapy, as the effective supplement oxygen flow decreased significantly (p=0.034 and 0.046 respectively for temporary positive expiratory pressure vs. positive expiratory pressure). In subjects on mechanical ventilation, positive expiratory pressure was superior to temporary positive expiratory pressure in increasing forced expiratory flow (p=0.018).
Conclusion: The physiological parameters of both groups improved significantly and similarly. Subgroup analysis suggests that temporary positive expiratory pressure could provide some advantage to subjects with emphysema and those on oxygen therapy, while positive expiratory pressure would benefit patients on mechanical ventilation. Randomized clinical trials are necessary to confirm our preliminary results indicating that different subgroups/phenotypes can benefit more from one type of treatment.
Keywords: Airway clearance techniques; Bronchiectasis; COPD; Chronic bronchitis; Pulmonary rehabilitation; TPEP.
Copyright © 2017 Associação Brasileira de Pesquisa e Pós-Graduação em Fisioterapia. Publicado por Elsevier Editora Ltda. All rights reserved.
Figures


Similar articles
-
Efficacy of temporary positive expiratory pressure (TPEP) in patients with lung diseases and chronic mucus hypersecretion. The UNIKO® project: a multicentre randomized controlled trial.Clin Rehabil. 2013 Apr;27(4):336-46. doi: 10.1177/0269215512458940. Epub 2012 Sep 11. Clin Rehabil. 2013. PMID: 22967853 Clinical Trial.
-
Comparison of intermittent positive pressure breathing and temporary positive expiratory pressure in patients with severe chronic obstructive pulmonary disease.Arch Bronconeumol. 2014 Jan;50(1):18-24. doi: 10.1016/j.arbres.2013.07.019. Epub 2013 Dec 8. Arch Bronconeumol. 2014. PMID: 24321380 Clinical Trial. English, Spanish.
-
[The effects of extrinsic positive end-expiratory pressure on work of breathing in patients with chronic obstructive pulmonary disease].Zhonghua Nei Ke Za Zhi. 2001 Jun;40(6):385-9. Zhonghua Nei Ke Za Zhi. 2001. PMID: 11798603 Chinese.
-
Noninvasive clearance of airway secretions.Respir Care Clin N Am. 1996 Jun;2(2):323-45. Respir Care Clin N Am. 1996. PMID: 9390886 Review.
-
[Physiopathology of acute respiratory failure in COPD and asthma].Minerva Anestesiol. 2001 Apr;67(4):198-205. Minerva Anestesiol. 2001. PMID: 11376510 Review. Italian.
Cited by
-
Systematic Review and Meta-Analysis of the Application of T-PEP in the Therapeutic Management of COPD Patients.J Clin Med. 2025 Jan 7;14(2):320. doi: 10.3390/jcm14020320. J Clin Med. 2025. PMID: 39860328 Free PMC article. Review.
-
Advancing the Battle against Cystic Fibrosis: Stem Cell and Gene Therapy Insights.Curr Med Sci. 2024 Dec;44(6):1155-1174. doi: 10.1007/s11596-024-2936-5. Epub 2024 Dec 16. Curr Med Sci. 2024. PMID: 39676146 Review.
-
Nursing Process Related to the Nursing Focus "Airway Clearance": A Scoping Review.Nurs Rep. 2024 Jul 31;14(3):1871-1896. doi: 10.3390/nursrep14030140. Nurs Rep. 2024. PMID: 39189270 Free PMC article.
-
Measuring airway clearance outcomes in bronchiectasis: a review.Eur Respir Rev. 2020 Apr 29;29(156):190161. doi: 10.1183/16000617.0161-2019. Print 2020 Jun 30. Eur Respir Rev. 2020. PMID: 32350088 Free PMC article. Review.
-
Airway Clearance Techniques: The Right Choice for the Right Patient.Front Med (Lausanne). 2021 Feb 4;8:544826. doi: 10.3389/fmed.2021.544826. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33634144 Free PMC article. Review.
References
-
- Nici L., Donner C., Wouters E. American Thoracic Society/European Respiratory Society Statement on Pulmonary Rehabilitation. Am J Respir Crit Care Med. 2006;173(12):1390–1413. - PubMed
-
- Prescott E., Lange P., Vestbo J. Chronic mucus hypersecretion in COPD and death from pulmonary infection. Eur Respir J. 1994;8(8):1333–1338. - PubMed
-
- Vestbo J., Prescott E., Lange P. Association of chronic mucus hypersecretion with FEV1 decline and chronic obstructive pulmonary disease morbidity. Copenhagen City Heart Study Group. Am J Respir Crit Care Med. 1996;153(5):1530–1535. - PubMed
-
- American Thoracic Society; New York, NY: 2012. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. [December 14]
-
- Vestbo J., Hurd S.S., Agustí A.G. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(4):347–365. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
