

Effect of intranasal dexmedetomidine on emergence agitation after sevoflurane anesthesia in children undergoing tonsillectomy and/or adenoidectomy
- PMID: 28442950
- PMCID: PMC5389230
- DOI: 10.4103/1658-354X.203020
Effect of intranasal dexmedetomidine on emergence agitation after sevoflurane anesthesia in children undergoing tonsillectomy and/or adenoidectomy
Abstract
Background: Emergence agitation (EA) after sevoflurane anesthesia is common in children during recovery from general anesthesia and may result in postoperative complications. This study investigated safety and effectiveness of intranasal dexmedetomidine in reducing the incidence and severity of EA.
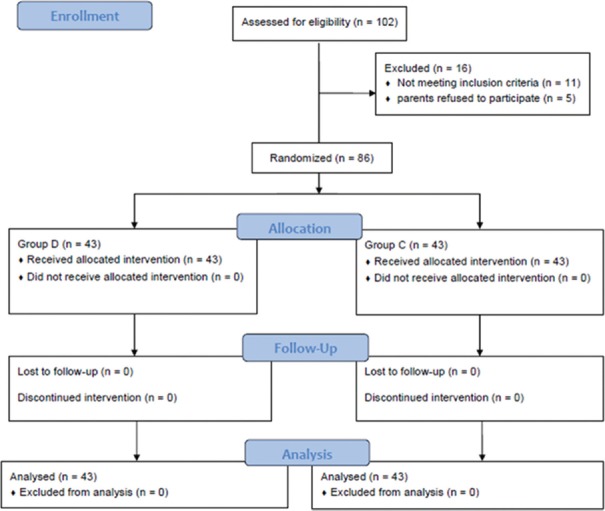
Methods: This prospective, randomized double-blinded controlled trial included 86 patients scheduled for the tonsillectomy and/or adenoidectomy under general anesthesia with sevoflurane. They were randomly allocated into two groups. Group D received intranasal dexmedetomidine at 1 μg/kg, and Group C received intranasal saline 0.9% after the induction of general anesthesia. Four-point agitation scale and Face, Legs, Activity, Cry and Consolability (FLACC) scale for pain assessment were measured at six time points (after extubation, leaving the operating room, on arrival to postanesthesia care unit [PACU], 10, 20, and 30 min after arrival in PACU). Extubation, emergence, and discharge times were recorded in addition to any adverse effects.
Results: There was a significant difference in the incidence of EA between Groups D and C (6.98% and 58%, respectively, with P = 0.001). The median four-point agitation scales and the median scores of FLACC pain scales of Group D were significantly lower than those of Group C at the all six time points with P < 0.05. Extubation, emergence, and discharge times were comparable in both groups, and none of the subjects reported any adverse effects.
Conclusion: This study demonstrates that a 1 μg/kg dose of intranasal dexmedetomidine administered after the induction of anesthesia reduces post-sevoflurane incidence and severity of EA in children undergone tonsillectomy and/or adenoidectomy with no adverse effects and smooth recovery profile.
Keywords: Dexmedetomidine; emergence agitation; sevoflurane; tonsillectomy and adenoidectomy.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Mountain BW, Smithson L, Cramolini M, Wyatt TH, Newman M. Dexmedetomidine as a pediatric anesthetic premedication to reduce anxiety and to deter emergence delirium. AANA J. 2011;79:219–24. - PubMed
-
- Vlajkovic GP, Sindjelic RP. Emergence delirium in children: Many questions, few answers. Anesth Analg. 2007;104:84–91. - PubMed
-
- Kuratani N, Oi Y. Greater incidence of emergence agitation in children after sevoflurane anesthesia as compared with halothane: A meta-analysis of randomized controlled trials. Anesthesiology. 2008;109:225–32. - PubMed
-
- Yassin H, Boules M. Comparative study between the effect of propofol and fentanyl on the incidence and severity of emergence agitation after sevoflurane anesthesia in pediatrics. Ain Shams J Anesthesiol. 2015;8:529–34.
-
- Patel A, Davidson M, Tran MC, Quraishi H, Schoenberg C, Sant M, et al. Dexmedetomidine infusion for analgesia and prevention of emergence agitation in children with obstructive sleep apnea syndrome undergoing tonsillectomy and adenoidectomy. Anesth Analg. 2010;111:1004–10. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
