

Initial single-centre Canadian experience with 18F-fluoromethylcholine positron emission tomography-computed tomography (18F-FCH PET/CT) for biochemical recurrence in prostate cancer patients initially treated with curative intent
- PMID: 28443145
- PMCID: PMC5403679
- DOI: 10.5489/cuaj.4068
Initial single-centre Canadian experience with 18F-fluoromethylcholine positron emission tomography-computed tomography (18F-FCH PET/CT) for biochemical recurrence in prostate cancer patients initially treated with curative intent
Abstract
Introduction: We sought to determine predictive factors (patient and prostate-specific antigen [PSA] characteristics) for 18F-fluoromethylcholine positron emission tomography-computed tomography (18F-FCH PET/CT) positivity in the context of biochemical recurrence after local treatment of prostate cancer (PCa) with curative intent.
Methods: This is a retrospective study including 60 18F-FCH PET/CT scans of patients with biochemical recurrence after initial radical prostatectomy (RP), external beam radiation therapy (EBRT), or focal high-intensity focused ultrasound (HIFU) with curative intent. The results were compared to findings on magnetic resonance imaging (MRI), computed tomography (CT), bone scan (BS), and histological analysis when available. Univariate analysis was performed to correlate results with patient characteristics.
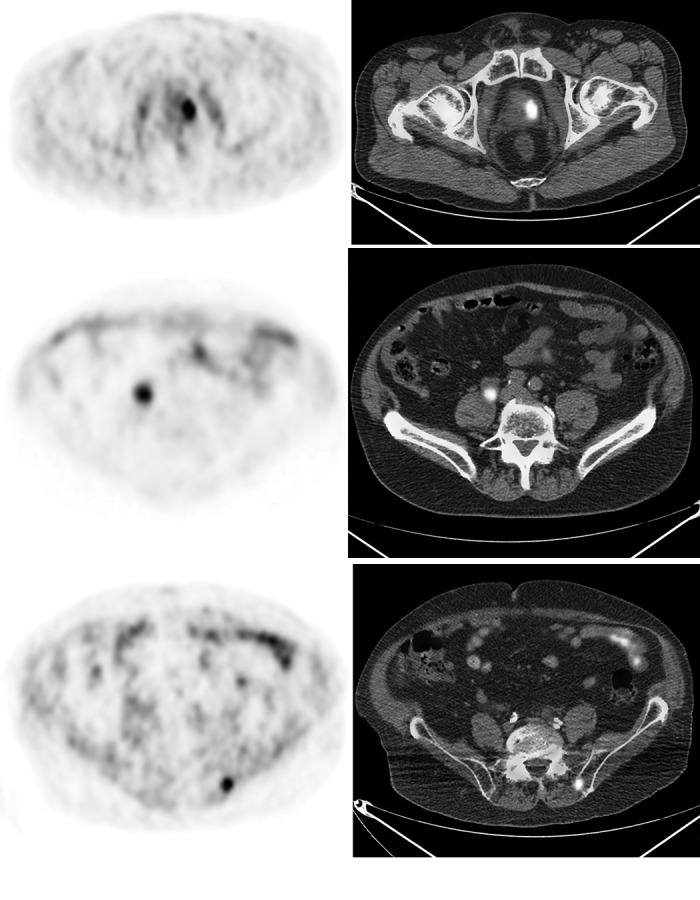
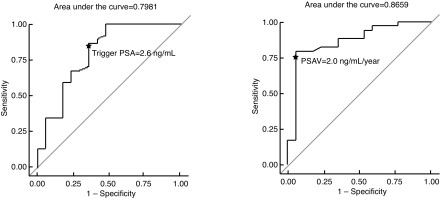
Results: Thirty-eight (63.3%) scans were positive, 17 (28.3%) negative, and 5 (8.3%) equivocal. Of the positive scans, 16 demonstrated local recurrence, 12 regional/distant lymph nodes, five bone metastasis, and five local and distant recurrences. Among the 22 PET/CTs showing metastasis, conventional imaging was performed in 16 patients (72.7%). Of these, it demonstrated the lesion(s) found on PET/CT in eight patients (50.0%), was negative in seven (43.8%), and equivocal in one (6.3%). The trigger PSA (p=0.04), prostate-specific antigen velocity (PSAV) (p=0.03), and prostate-specific antigen doubling time (PSADT) (p=0.046) were significantly different when comparing positive and negative scans. Patients with positive scans were more likely to have received EBRT initially (odds ratio [OR] 11.0, 95% confidence interval [CI] 2.2-55.3). A trigger PSA of 2.6 ng/mL had a sensitivity of 84% and specificity of 65% for a positive scan. PET/CT changed the clinical management plan in 17 patients (28.3%).
Conclusions: 18F-FCH PET/CT demonstrates a high detection rate for local and distant recurrences after localized PCa treatment. A trigger PSA above 2.6 ng/mL seems optimal for appropriate patient selection.
Figures
References
-
- Cancer.ca. Canadian Cancer Society’s Advisory Committee on Cancer Statistics; 2015. [updated 2015; cited 2016 February 17]. http://www.cancer.ca/. Accessed February 17, 2016.
-
- Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol. 2014;65:124–37. https://doi.org/10.1016/j.eururo.2013.09.046. - DOI - PubMed
-
- Shah TT, Kasivisvanathan V, Jameson C, et al. Histological outcomes after focal high-intensity focused ultrasound and cryotherapy. World J Urol. 2015;33:955–64. https://doi.org/10.1007/s00345-015-1561-0. - DOI - PMC - PubMed
-
- Valerio M, Ahmed HU, Emberton M, et al. The role of focal therapy in the management of localised prostate cancer: A systematic review. Eur Urol. 2014;66:732–51. https://doi.org/10.1016/j.eururo.2013.05.048. - DOI - PMC - PubMed
-
- Han M, Partin AW, Pound CR, et al. Long-term biochemical disease-free and cancer-specific survival following anatomic radical retropubic prostatectomy. The 15-year Johns Hopkins experience. Urol Clin North Am. 2001;28:555–65. https://doi.org/10.1016/S0094-0143(05)70163-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
