

Childhood Sustained Hypercalcemia: A Diagnostic Challenge
- PMID: 28443817
- PMCID: PMC5785637
- DOI: 10.4274/jcrpe.4247
Childhood Sustained Hypercalcemia: A Diagnostic Challenge
Abstract
Objective: This study aimed to call attention to hypercalcemia, a rare finding in children which carries the potential of leading to serious complications without proper intervention.
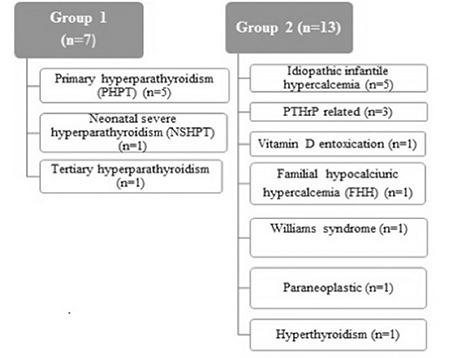
Methods: Diagnosis, treatment, and clinical course of children with sustained hypercalcemia admitted between the years 2006-2016 were reviewed. Group 1 [parathyroid hormone (PTH)-dependent] consisted of patients with high/unsuppressed PTH levels and group 2 (PTH-independent) included cases with normal/suppressed PTH levels.
Results: Twenty patients (11 male, 9 female) with a median age of 6.25 (0.03-17.88) years were evaluated. Symptoms were mostly related with the gastrointestinal system, while six patients (30%) were asymptomatic. Physical examination findings were diverse, non-specific, and normal in four patients (20%). Median time of diagnosis was 45 (2-720) days. Patients were divided into group 1 (n=7) and group 2 (n=13). Most frequent etiologies were primary hyperparathyroidism (n=5), idiopathic infantile hypercalcemia (IIH) (n=5), and malignancy (n=4). A moderate positive correlation was noted between serum calcium and creatinine levels (r=0.53, p=0.02). Nephrocalcinosis was the most common complication (n=9) (45%). Treatment was not implemented in 2 patients with mild hypercalcemia, while other patients received medical treatment ± surgery. Treatment-resistant patients were cases of malignancies and neonatal severe hyperparathyroidism. Long-term follow-up displayed resistant hypercalciuria in three infants diagnosed as IIH.
Conclusion: Many patients with childhood hypercalcemia are asymptomatic or exhibit a non-specific and heterogeneous clinical presentation, resulting in delayed diagnosis. Mild cases may not be recognized, while symptoms may be missed in the presence of accompanying illnesses. Nevertheless, serious complications may only be avoided with prompt diagnosis and intervention.
Keywords: Hypercalcemia; hyperparathyroidism; idiopathic infantile hypercalcemia; malignancy-related hypercalcemia pediatrics..
Figures
References
-
- Rodd C, Goodyer P. Hypercalcemia of the newborn: etiology, evaluation, and management. Pediatr Nephrol. 1999;13:542–547. - PubMed
-
- Davies JH. Approach to the Child with Hypercalcaemia. Endocr Dev. 2015;28:101–118. - PubMed
-
- Davies JH, Shaw NJ. Investigation and management of hypercalcaemia in children. Arch Dis Child. 2012;97:533–538. - PubMed
-
- Mallet E Working Group on Calcium Metabolism. Primary hyperparathyroidism in neonates and childhood. The French experience (1984-2004) Horm Res. 2008;69:180–188. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous