

Shortening cardioplegic arrest time in patients undergoing combined coronary and valve surgery: results from a multicentre randomized controlled trial: the SCAT trial
- PMID: 28444178
- PMCID: PMC5848808
- DOI: 10.1093/ejcts/ezx087
Shortening cardioplegic arrest time in patients undergoing combined coronary and valve surgery: results from a multicentre randomized controlled trial: the SCAT trial
Abstract
Objectives: Combined coronary artery bypass grafting and valve surgery requires a prolonged period of cardioplegic arrest (CA) predisposing to myocardial injury and postoperative cardiac-specific complications. The aim of this trial was to reduce the CA time in patients undergoing combined coronary artery bypass grafting and valve surgery and assess if this was associated with less myocardial injury and related complications.
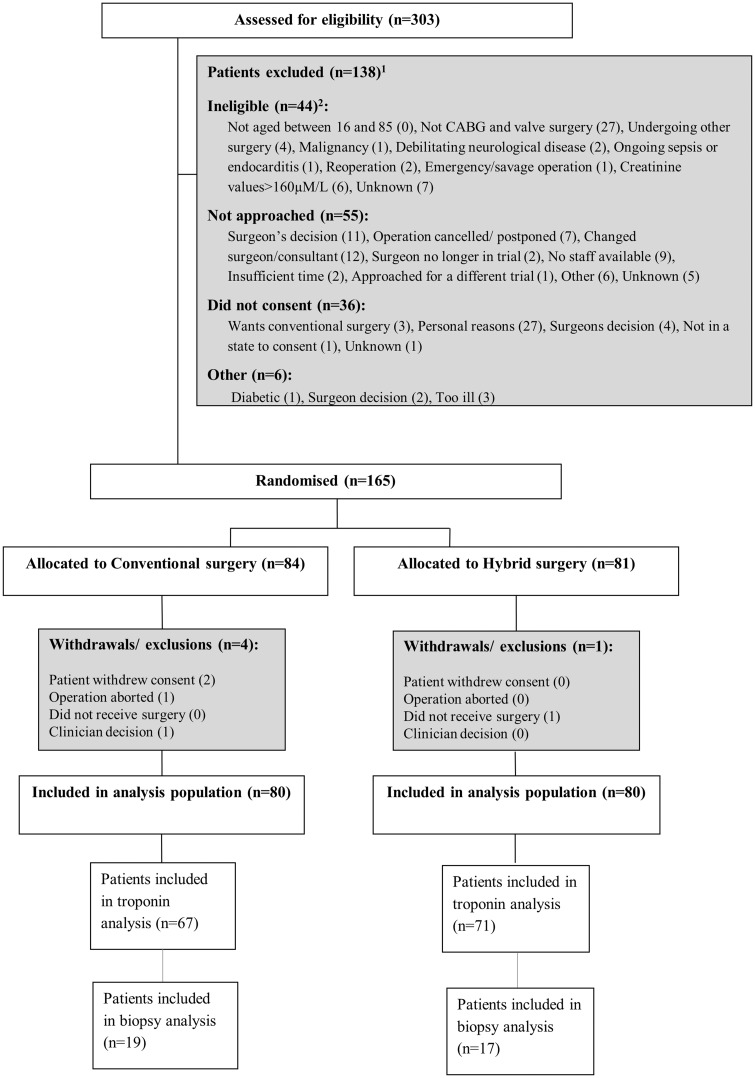
Methods: Participants were randomized to (i) coronary artery bypass grafting performed on the beating heart with cardiopulmonary bypass support followed by CA for the valve procedure (hybrid) or (ii) both procedures under CA (conventional). To assess complications related to myocardial injury, we used the composite of death, myocardial infarction, arrhythmia, need for pacing or inotropes for >12 h. To assess myocardial injury, we used serial plasma troponin T and markers of metabolic stress in myocardial biopsies.
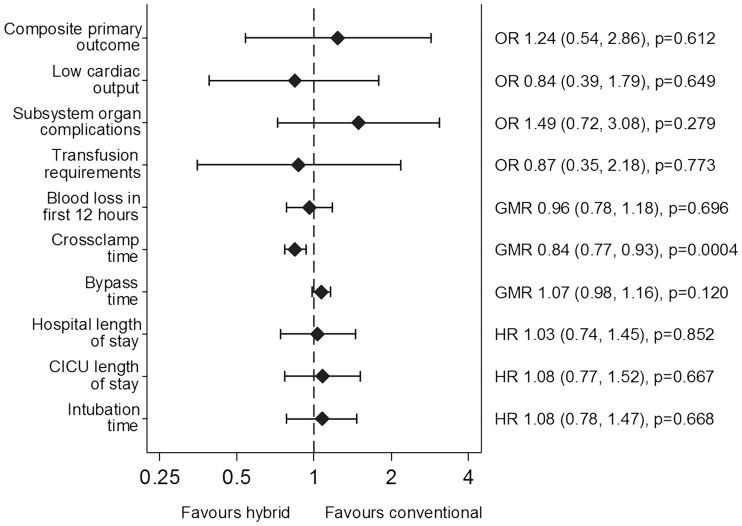
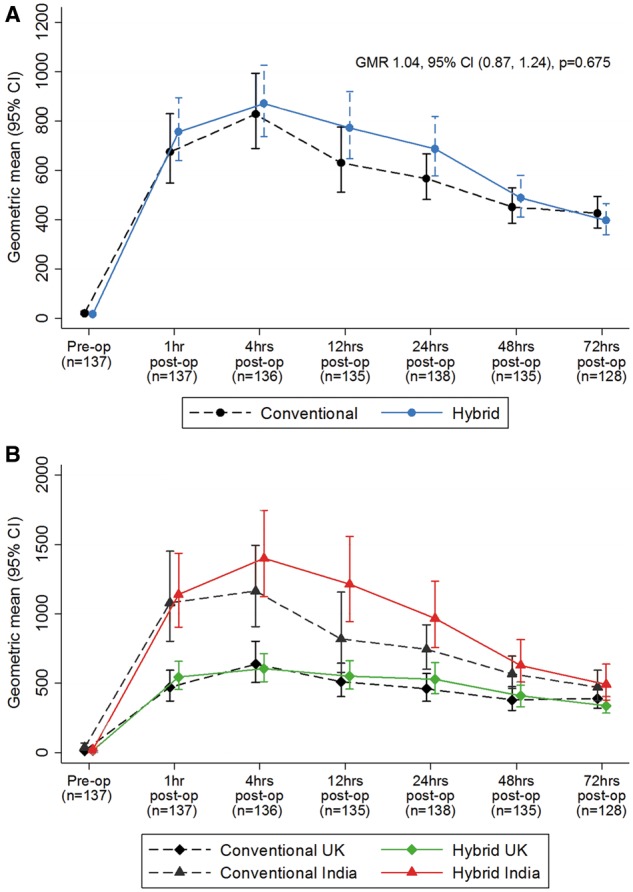
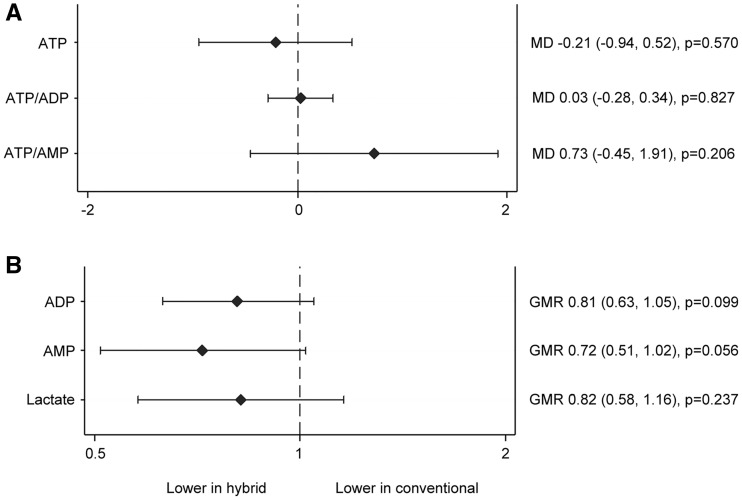
Results: Hundred and sixty patients (80 hybrid and 80 conventional) were randomized. Mean age was 66.5 years and 74% were male. Valve procedures included aortic (61.8%) and mitral (33.1%) alone or in combination (5.1%). CA time was 16% lower in the hybrid group [median 98 vs 89 min, geometric mean ratio (GMR) 0.84, 95% confidence interval (CI) 0.77-0.93, P = 0.0004]. Complications related to myocardial injury occurred in 131/160 patients (64/80 conventional, 67/80 hybrid), odds ratio 1.24, 95% CI 0.54-2.86, P = 0.61. Release of troponin T was similar between groups (GMR 1.04, 95% CI 0.87-1.24, P = 0.68). Adenosine monophosphate was 28% lower in the hybrid group (GMR 0.72, 95% CI 0.51-1.02, P = 0.056).
Conclusions: The hybrid procedure reduced the CA time but myocardial injury outcomes were not superior to conventional approach.
Trial registration: ISRCTN65770930.
Keywords: Beating heart coronary surgery; Cardioplegic arrest; Myocardial protection; Valve surgery.
© The Author 2017. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Bridgewater B, Keogh B, Kinsman R, Walton P.. Sixth National Adult Cardiac Surgical Database Report, 2008. http://www.scts.org/_userfiles/resources/SixthNACDreport2008withcovers.org.
-
- Buth KJ, Gainer RA, Legare JF, Hirsch GM.. The changing face of cardiac surgery: practice patterns and outcomes 2001-2010. Can J Cardiol 2014;30:224–30. - PubMed
-
- Keogh B, Kinsman R.. National Adult Cardiac Surgical Database 1999–2000. Dendrite Clinical Systems/ The Society of Cardiothoracic Surgeons of Great Britain and Ireland, 2003.
-
- Edwards FH, Peterson ED, Coombs LP, DeLong ER, Jamieson WR, Shroyer ALW. et al. Prediction of operative mortality after valve replacement surgery. JACC 2001;37:885–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
