

Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel
- PMID: 28444290
- PMCID: PMC5837225
- DOI: 10.1093/eurheartj/ehx144
Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel
Abstract
Aims: To appraise the clinical and genetic evidence that low-density lipoproteins (LDLs) cause atherosclerotic cardiovascular disease (ASCVD).
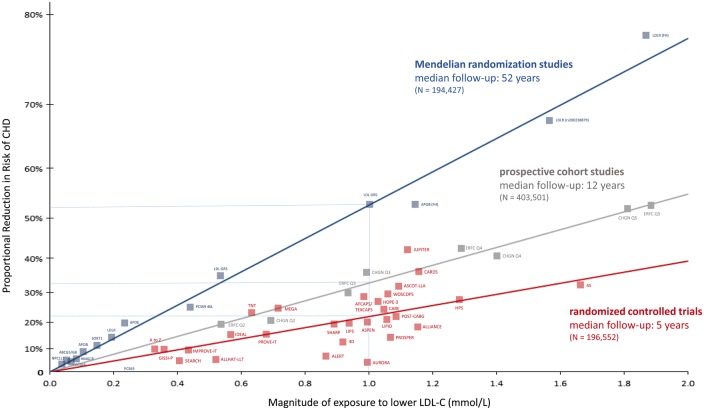
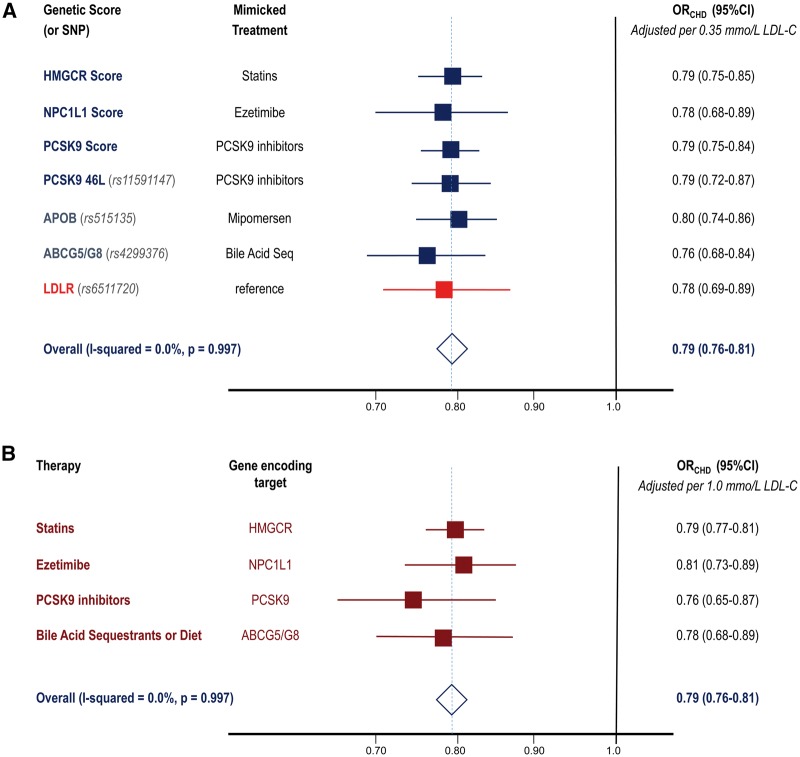
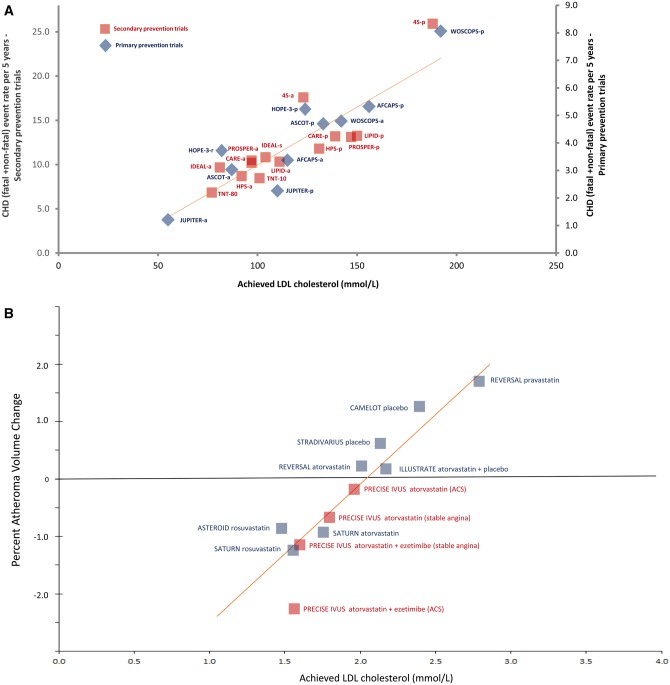
Methods and results: We assessed whether the association between LDL and ASCVD fulfils the criteria for causality by evaluating the totality of evidence from genetic studies, prospective epidemiologic cohort studies, Mendelian randomization studies, and randomized trials of LDL-lowering therapies. In clinical studies, plasma LDL burden is usually estimated by determination of plasma LDL cholesterol level (LDL-C). Rare genetic mutations that cause reduced LDL receptor function lead to markedly higher LDL-C and a dose-dependent increase in the risk of ASCVD, whereas rare variants leading to lower LDL-C are associated with a correspondingly lower risk of ASCVD. Separate meta-analyses of over 200 prospective cohort studies, Mendelian randomization studies, and randomized trials including more than 2 million participants with over 20 million person-years of follow-up and over 150 000 cardiovascular events demonstrate a remarkably consistent dose-dependent log-linear association between the absolute magnitude of exposure of the vasculature to LDL-C and the risk of ASCVD; and this effect appears to increase with increasing duration of exposure to LDL-C. Both the naturally randomized genetic studies and the randomized intervention trials consistently demonstrate that any mechanism of lowering plasma LDL particle concentration should reduce the risk of ASCVD events proportional to the absolute reduction in LDL-C and the cumulative duration of exposure to lower LDL-C, provided that the achieved reduction in LDL-C is concordant with the reduction in LDL particle number and that there are no competing deleterious off-target effects.
Conclusion: Consistent evidence from numerous and multiple different types of clinical and genetic studies unequivocally establishes that LDL causes ASCVD.
Keywords: Atherosclerosis; Cardiovascular disease; Causality; Clinical trials; Ezetimibe; Low-density lipoprotein; Mendelian randomization; PCSK9; Recommendations; Statin.
© The Author 2017. Published on behalf of the European Society of Cardiology
Figures
Comment in
-
Evolocumab and clinical outcomes in patients with cardiovascular disease.J R Coll Physicians Edinb. 2017 Jun;47(2):153-155. doi: 10.4997/JRCPE.2017.212. J R Coll Physicians Edinb. 2017. PMID: 28675189 No abstract available.
References
-
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L; INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004;364:937–952. - PubMed
-
- DuBroff R. Cholesterol paradox: a correlate does not a surrogate make. Evid Based Med 2017;22:15–19. - PubMed
-
- Ravnskov U, Diamond DM, Hama R, Hamazaki T, Hammarskjöld B, Hynes N, Kendrick M, Langsjoen PH, Malhotra A, Mascitelli L, McCully KS, Ogushi Y, Okuyama H, Rosch PJ, Schersten T, Sultan S, Sundberg R.. Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review. BMJ Open 2016;6:e010401. - PMC - PubMed
-
- Camejo G, Lopez A, Vegas H, Paoli H.. The participation of aortic proteins in the formation of complexes between low density lipoproteins and intima-media extracts. Atherosclerosis 1975;21:77–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
- Archivio Istituzionale della Ricerca Unimi - Access Free Full Text
- Enlighten: Publications, University of Glasgow - Access Free Full Text
- Europe PubMed Central
- Ovid Technologies, Inc.
- PubMed Central
- Silverchair Information Systems
- Spiral, Imperial College Digital Repository
- eScholarship, University of California - Access Free Full Text
Other Literature Sources
Medical
Miscellaneous
