

Endometrial cancer arising in adenomyosis versus endometrial cancer coexisting with adenomyosis: are these two different entities?
- PMID: 28444512
- PMCID: PMC7523234
- DOI: 10.1007/s00404-017-4375-z
Endometrial cancer arising in adenomyosis versus endometrial cancer coexisting with adenomyosis: are these two different entities?
Abstract
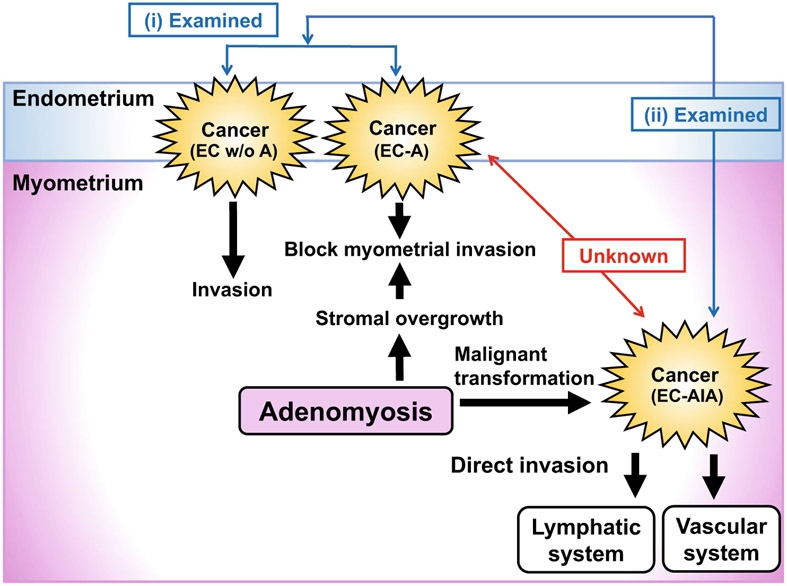
Purpose: While adenomyosis is one of the most common benign histologic findings in hysterectomy specimens of endometrial cancer, demographics of endometrial cancer arising in adenomyosis (EC-AIA) has not been well elucidated. The aim of this study is to evaluate histopathological findings and disease-free survival (DFS) of EC-AIA in comparison to endometrial cancer coexisting with adenomyosis (EC-A).
Methods: EC-AIA cases were identified via a systematic literature search (n = 46). EC-A cases were identified from a historical cohort that underwent hysterectomy-based surgical staging in two institutions (n = 350). Statistical comparisons of the two groups were based on univariate and multivariate analyses.
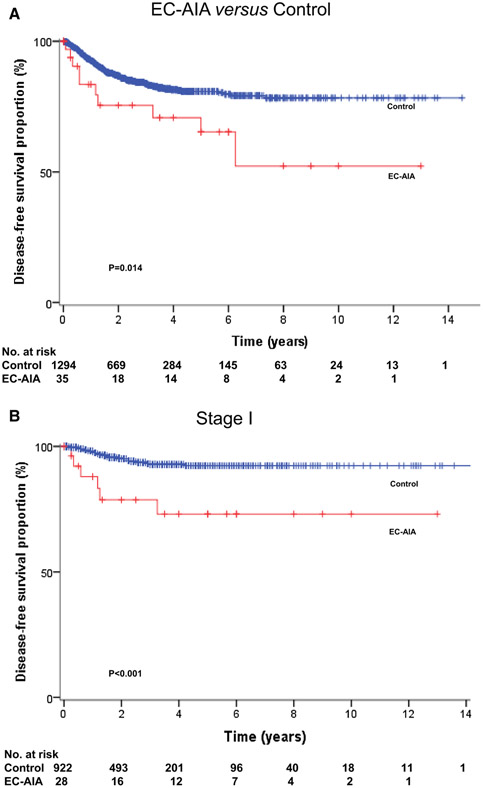
Results: The EC-AIA group was significantly older than the EC-A group (58.9 versus 53.8, p = 0.002). As to tumor characteristics, 63.6% of EC-AIA cases reported tumor within the myometrium without endometrial extension. The EC-AIA group was significantly associated with more non-endometrioid histology (23.9 versus 14.8%; p = 0.002) and deep myometrial tumor invasion (51.6 versus 19.4%; p < 0.001) than EC-A. Tumor grade, stage, and nodal metastasis risk were similar (all, p > 0.05). In a univariate analysis, the EC-AIA group had a significantly decreased DFS compared to EC-A (5-year rates, 72.2 versus 85.5%, p = 0.001). After controlling for age, histology, tumor grade, and stage, EC-AIA remained an independent prognostic factor associated with decreased DFS compared to EC-A (adjusted-hazard ratio 2.87, 95% confidence interval 1.44-5.70, p = 0.031).
Conclusion: Our study demonstrated that EC-AIA has distinct tumor characteristics and a poorer survival outcome compared to EC-A. This suggests a benefit of recognition of this unique entity as an aggressive variant of endometrial cancer.
Keywords: Adenomyosis; Endometrial cancer; Endometriosis-associated cancer; Prognosis; Survival.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A (2017) Cancer statistics. CA Cancer J Clin 67:7–30 - PubMed
-
- [Accessed 27 Jan 2016]; http://seer.cancer.gov/statfacts/html/corp.html.
-
- Ferenczy A (1998) Pathophysiology of adenomyosis. Hum Reprod Update 4:312–322 - PubMed
-
- Vercellini P, Vigano P, Somigliana E et al. (2006) Adenomyosis: epidemiological factors. Best Pract Res Clin Obstet Gynaecol 20:465–477 - PubMed
-
- Kairi-Vassilatou E, Kontogianni K, Salamalekis M et al. (2004) A clinicopathological study of the relationship between adenomyosis and other hormone-dependent uterine lesions. Eur J Gynaecol Oncol 25:222–224 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
