

An economic evaluation of the Enhanced Recovery After Surgery (ERAS) multisite implementation program for colorectal surgery in Alberta
- PMID: 28445024
- PMCID: PMC5125924
- DOI: 10.1503/cjs.006716
An economic evaluation of the Enhanced Recovery After Surgery (ERAS) multisite implementation program for colorectal surgery in Alberta
Abstract
Background: In February 2013, Alberta Health Services established an Enhanced Recovery After Surgery (ERAS) implementation program for adopting the ERAS Society colorectal guidelines into 6 sites (initial phase) that perform more than 75% of all colorectal surgeries in the province. We conducted an economic evaluation of this initiative to not only determine its cost-effectiveness, but also to inform strategy for the spread and scale of ERAS to other surgical protocols and sites.
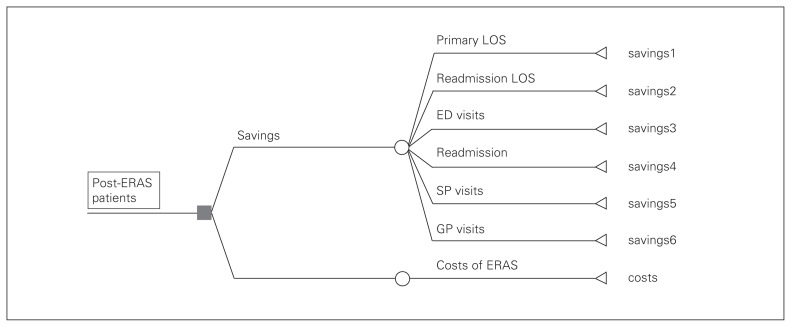
Methods: We assessed the impact of ERAS on patients’ health services utilization (HSU; length of stay [LOS], readmissions, emergency department visits, general practitioner and specialist visits) within 30 days of discharge by comparing pre- and post-ERAS groups using multilevel negative binomial regressions. We estimated the net health care costs/savings and the return on investment (ROI) associated with those impacts for post-ERAS patients using a decision analytic modelling technique.
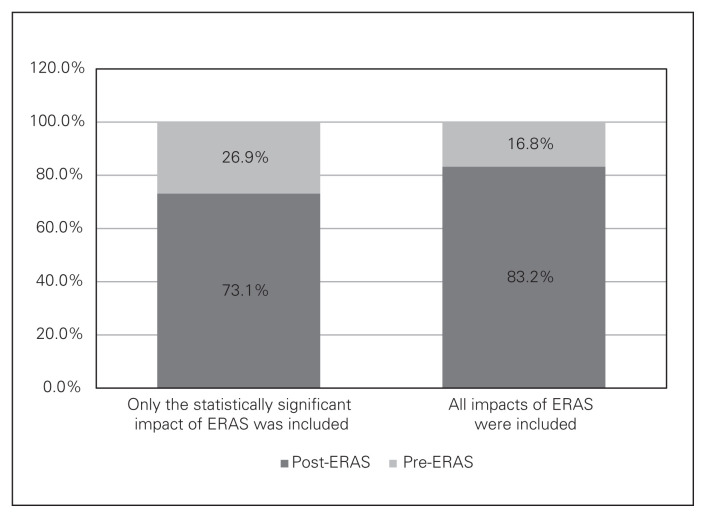
Results: We included 331 pre- and 1295 post-ERAS patients in our analyses. ERAS was associated with a reduction in all HSU outcomes except visits to specialists. However, only the reduction in primary LOS was significant. The net health system savings were estimated at $2 290 000 (range $1 191 000–$3 391 000), or $1768 (range $920–$2619) per patient. The probability for the program to be cost-saving was 73%–83%. In terms of ROI, every $1 invested in ERAS would bring $3.8 (range $2.4–$5.1) in return.
Conclusion: The initial phase of ERAS implementation for colorectal surgery in Alberta is cost-saving. The total savings has the potential to be more substantial when ERAS is spread for other surgical protocols and across additional sites.
Contexte: En février 2013, les Services de santé de l’Alberta ont mis en place le programme ERAS (Enhanced Recovery After Surgery — récupération postchirurgicale améliorée) dans le but de faire adopter les lignes directrices en matière d’interventions colorectales de la ERAS Society à 6 établissements (première phase) où sont prati-quées plus de 75 % des interventions chirurgicales colorectales de la province. Nous avons réalisé une évaluation économique du programme, non seulement pour en mesurer la rentabilité, mais aussi pour élaborer une stratégie visant à étendre le programme ERAS à d’autres protocoles chirurgicaux et services de chirurgie.
Méthodes: Nous avons mesuré les effets du programme ERAS sur l’utilisation des services de santé (durée de séjour, réadmissions, visites au service des urgences, visites d’un omnipraticien ou d’un spécialiste) dans les 30 jours suivant le congé en comparant les groupes pré- et post-ERAS à l’aide de régressions binomiales négatives multiniveaux. Nous avons évalué le coût net des soins de santé, les économies réalisées et le rendement sur investissement (RSI) associés aux mesures ci-dessus chez les patients post-ERAS à l’aide d’une technique de modélisation analytique décisionnelle.
Résultats: Nos analyses ont porté sur 331 patients pré-ERAS et 1295 patients post-ERAS. Nous avons observé une réduction de toutes les mesures de l’utilisation des services de santé étudiées, sauf les visites d’un spécialiste. Toutefois, seule la réduction de la durée du premier séjour était significative. Les économies nettes pour le système de santé ont été estimées à 2 290 000 $ (de 1 191 000 $ à 3 391 000 $), soit 1768 $ (de 920 $ à 2619 $) par patient. La probabilité que le programme soit économique était de 73 % à 83 %. En ce qui concerne le RSI, nous avons établi que chaque dollar investi dans le programme ERAS rapporterait 3,8 $ (de 2,4 $ à 5,1 $).
Conclusion: La première phase de la mise en oeuvre du programme ERAS en Alberta, appliqué à la chirurgie colorectale, a été économique. Les économies pour le système de santé pourraient être plus importantes si l’on étendait le programme à d’autres protocoles chirurgicaux et services de chirurgie.
Figures
References
-
- Fearon KCH, Ljungqvist O, Meyenfeldt MV, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24:466–77. - PubMed
-
- Roulin D, Donadini A, Gander S, et al. Cost-effectiveness of the implementation of an enhanced recovery protocol for colorectal surgery. Br J Surg. 2013;100:1108–14. - PubMed
-
- Bakker N, Cakir H, Doodeman HJ, et al. Eight years of experience with Enhanced Recovery After Surgery in patients with colon cancer: Impact of measures to improve adherence. Surgery. 2015;157:1130–6. - PubMed
-
- Ljungqvist O, Jonathan E. Rhoads lecture 2011: Insulin resistance and enhanced recovery after surgery. J Parenter Enteral Nutr. 2012;36:389–98. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources