

Single Delivery of High-Diversity Fecal Microbiota Preparation by Colonoscopy Is Safe and Effective in Increasing Microbial Diversity in Active Ulcerative Colitis
- PMID: 28445246
- PMCID: PMC6159890
- DOI: 10.1097/MIB.0000000000001132
Single Delivery of High-Diversity Fecal Microbiota Preparation by Colonoscopy Is Safe and Effective in Increasing Microbial Diversity in Active Ulcerative Colitis
Abstract
Background: Recent trials suggest fecal microbiota transplantation (FMT) with repeated enemas and high-diversity FMT donors is a promising treatment to induce remission in ulcerative colitis.
Methods: We designed a prospective, open-label pilot study to assess the safety, clinical efficacy, and microbial engraftment of single FMT delivery by colonoscopy for active ulcerative colitis using a 2-donor fecal microbiota preparation (FMP). Safety and clinical endpoints of response, remission, and mucosal healing at week 4 were assessed. Fecal DNA and rectal biopsies were used to characterize the microbiome and mucosal CD4 T cells, respectively, before and after FMT.
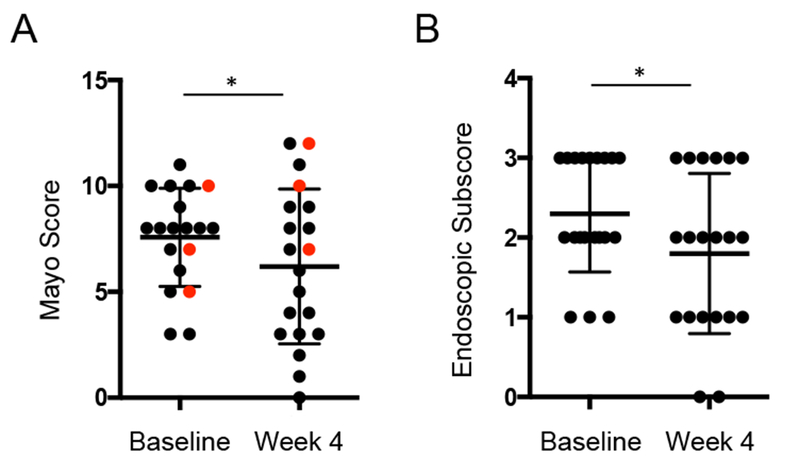
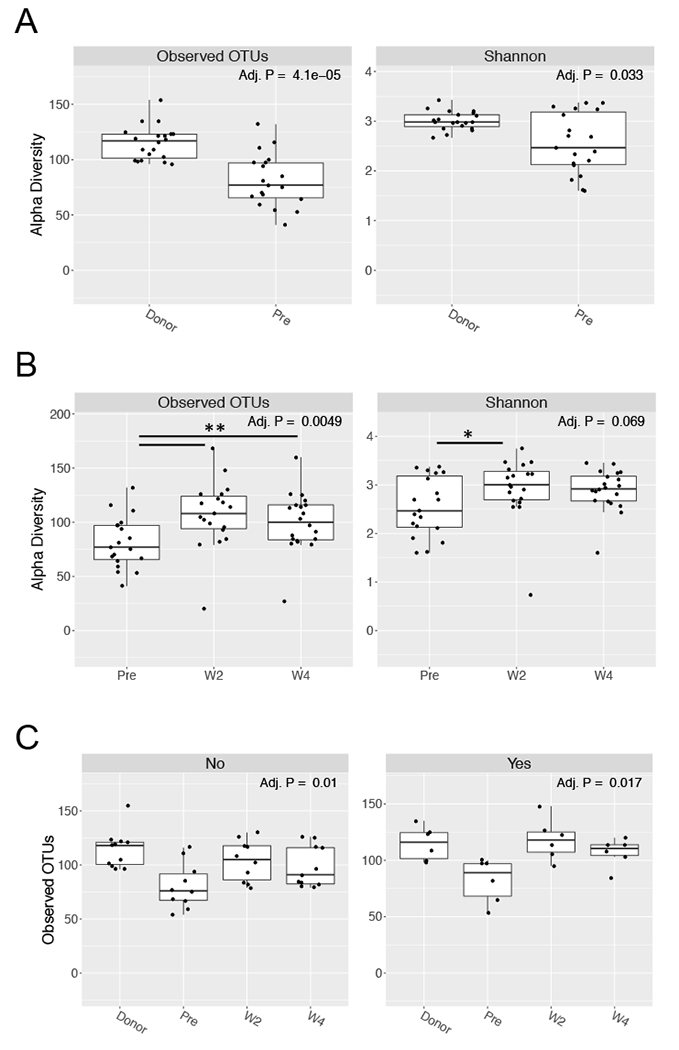
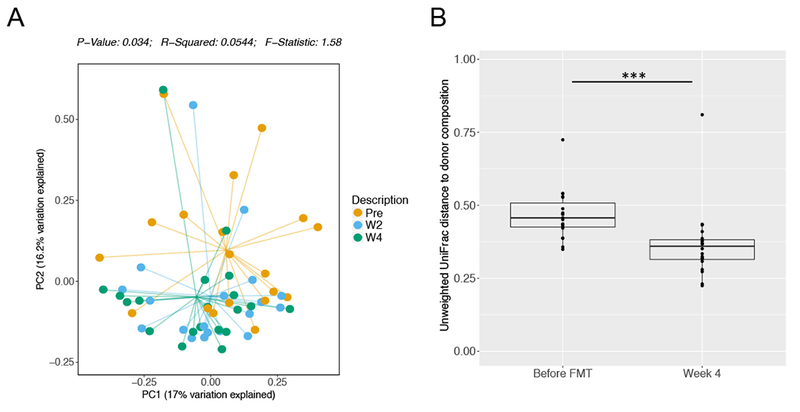
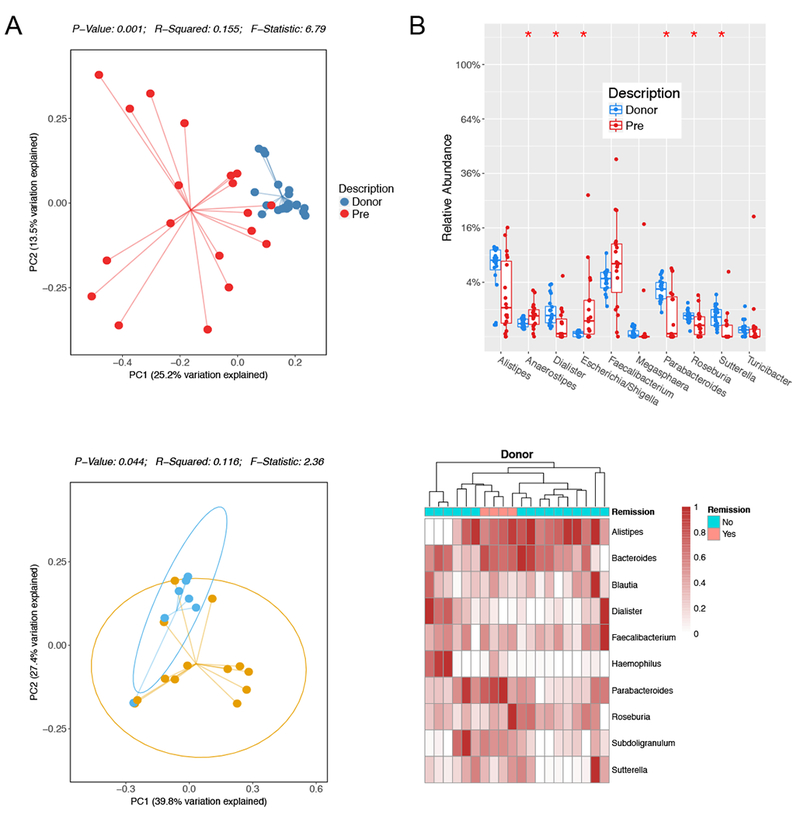
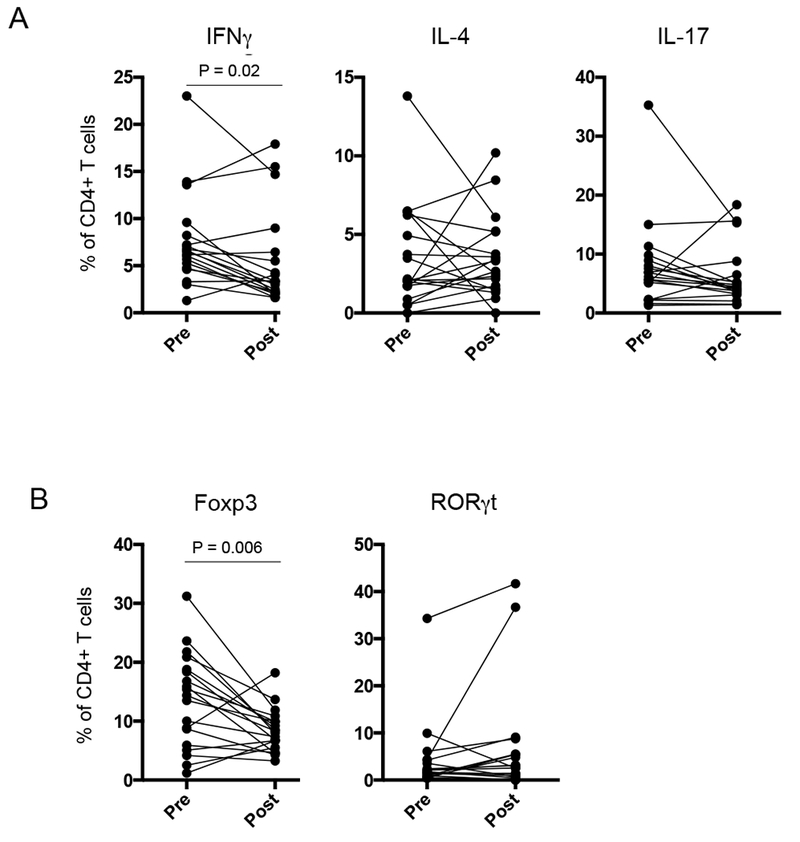
Results: Of the 20 patients enrolled in this study, 7 patients (35%) achieved a clinical response by week 4. Three patients (15%) were in remission at week 4 and 2 of these patients (10%) achieved mucosal healing. Three patients (15%) required escalation of care. No serious adverse events were observed. Microbiome analysis revealed that restricted diversity of recipients pre-FMT was significantly increased by high-diversity 2-donor FMP. The microbiome of recipients post-transplant was more similar to the donor FMP than the pretransplant recipient sample in both responders and nonresponders. Notably, donor composition correlated with clinical response. Mucosal CD4 T-cell analysis revealed a reduction in both Th1 and regulatory T-cells post-FMT.
Conclusions: High-diversity, 2-donor FMP delivery by colonoscopy seems safe and effective in increasing fecal microbial diversity in patients with active ulcerative colitis. Donor composition correlated with clinical response and further characterization of immunological parameters may provide insight into factors influencing clinical outcome.
Figures
References
-
- van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med. 2013;368:407–415 - PubMed
-
- Sartor RB. Microbial influences in inflammatory bowel diseases. Gastroenterology. 2008;134:577–594 - PubMed
-
- Rossen NG, Fuentes S, van der Spek MJ, et al. Findings From a Randomized Controlled Trial of Fecal Transplantation for Patients With Ulcerative Colitis. Gastroenterology. 2015;149:110–118 e114 - PubMed
-
- Moayyedi P, Surette MG, Kim PT, et al. Fecal Microbiota Transplantation Induces Remission in Patients With Active Ulcerative Colitis in a Randomized Controlled Trial. Gastroenterology. 2015;149:102–109 e106 - PubMed
-
- Kump PK, Grochenig HP, Lackner S, et al. Alteration of intestinal dysbiosis by fecal microbiota transplantation does not induce remission in patients with chronic active ulcerative colitis. Inflamm Bowel Dis. 2013;19:2155–2165 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
