

The effect of Timolol 0.5% on the correction of myopic regression after LASIK
- PMID: 28445315
- PMCID: PMC5413280
- DOI: 10.1097/MD.0000000000006782
The effect of Timolol 0.5% on the correction of myopic regression after LASIK
Abstract
Backgroud: Postlaser in situ keratomileusis (post-LASIK) refractive regression is defined as the gradual, partial, or total loss of initial correction that limits the predictability, efficiency, and long-term stability of LASIK. Our study assesses the effect of Timolol 0.5% on the correction of myopic regression after LASIK.
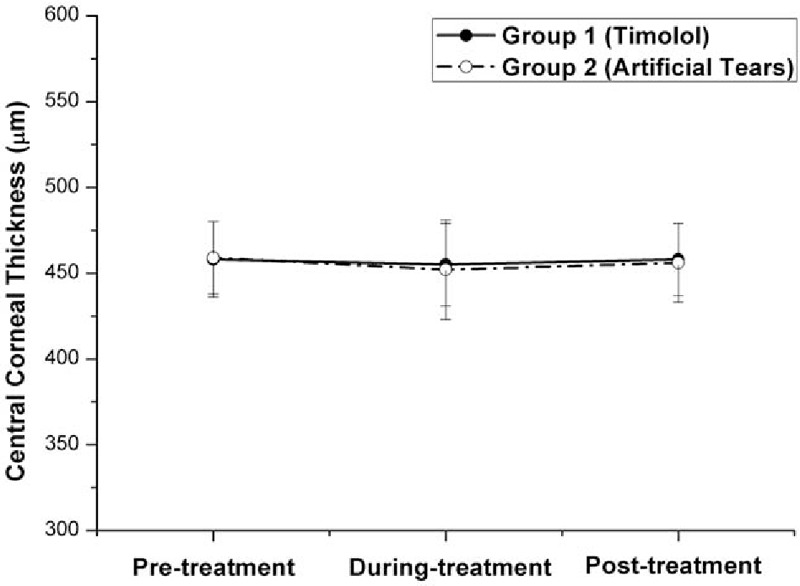
Methods: This prospective, randomized, controlled study included 62 eyes of 62 patients with myopic regression of -1.18 ± 0.86 diopters (D) after myopic LASIK. They were randomly assigned into either Group 1 who received Timolol 0.5% eye drops for 3 months or Group 2 who received artificial tears as control (during treatment). Patients were followed an additional 2 months after cessation of eye drops treatment (posttreatment).
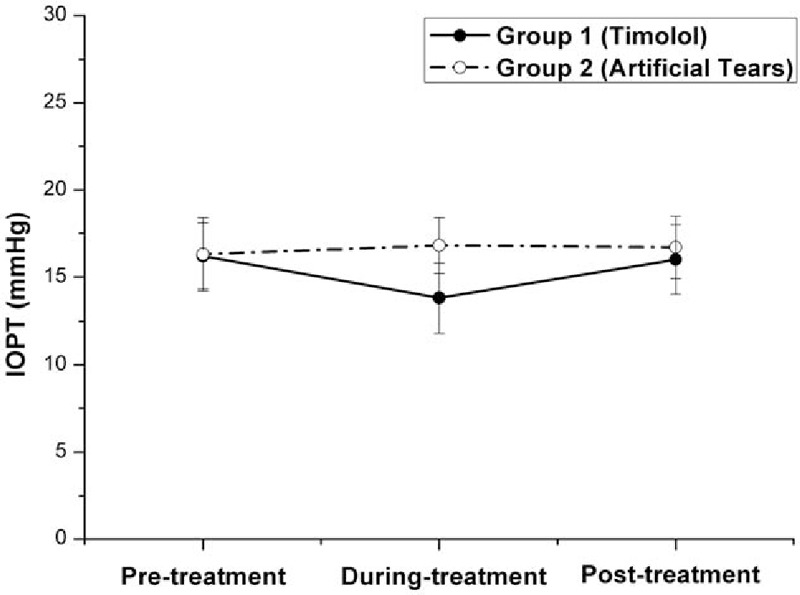
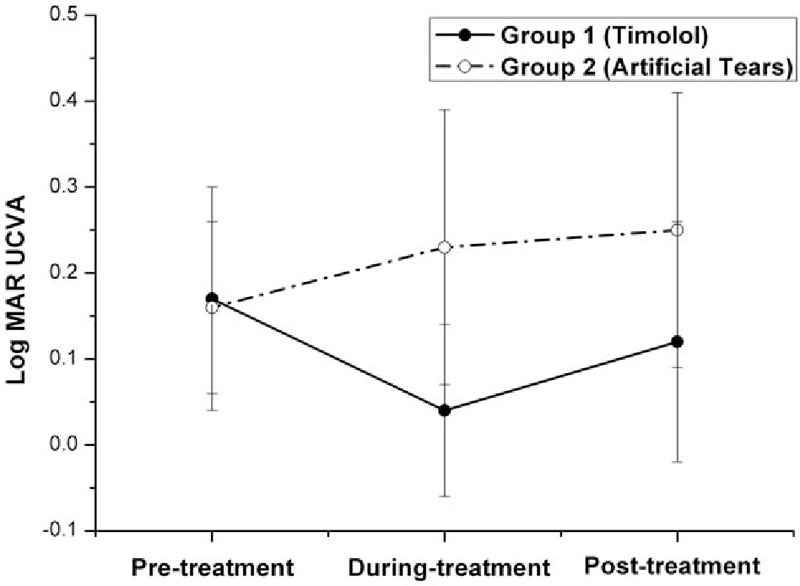
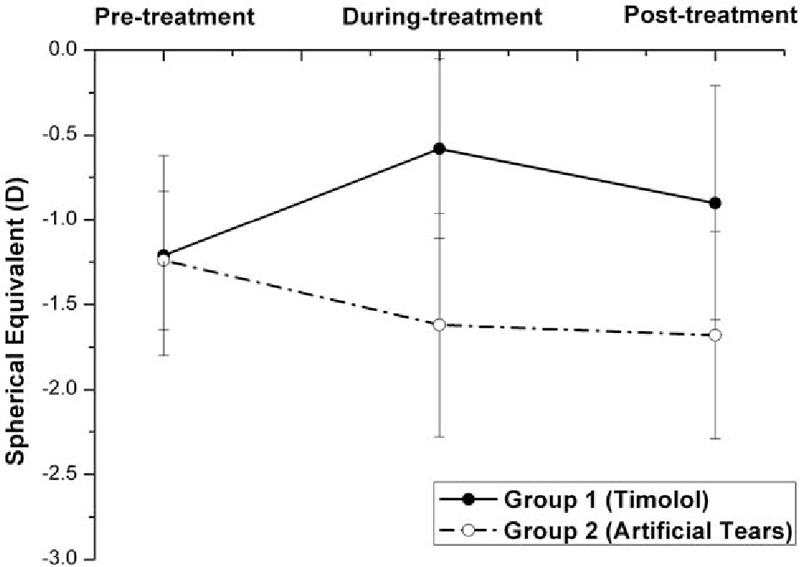
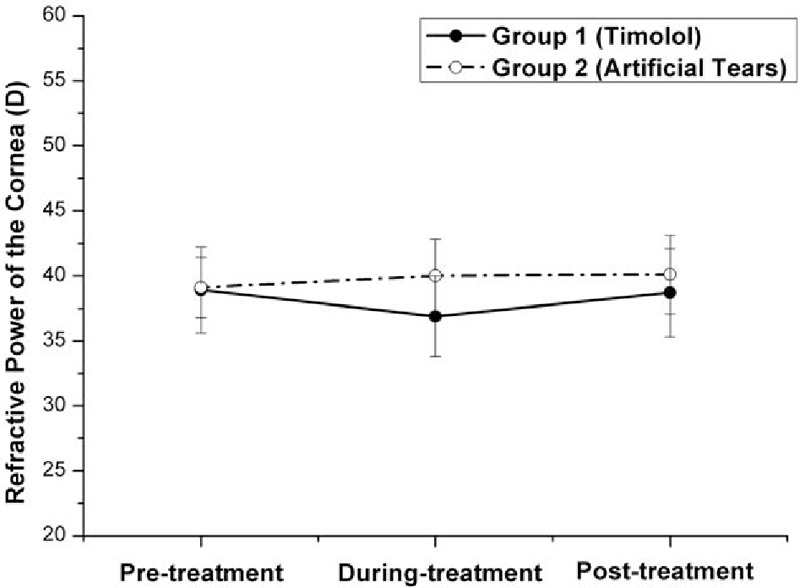
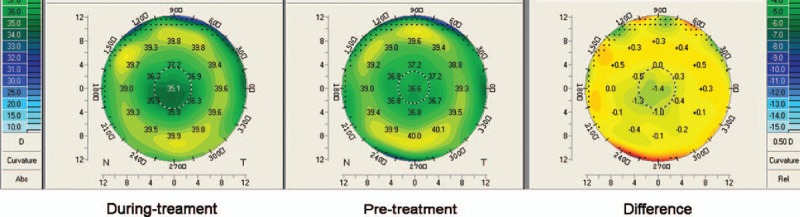
Results: During treatment in Group 1, as the mean true intraocular pressure (IOPT) lowered significantly, regression stopped. As the mean IOPT increased significantly posttreatment and returned to its pretreatment level, regression recurred. The effective rate of Timolol therapy dropped from 62.5% during treatment to 40.6% posttreatment. On the contrary in Group 2, although the mean IOPT did not change significantly, regression continually happened as time passed. During treatment, the mean IOPT, uncorrected visual acuity, spherical equivalent (SE), and corneal refractive power showed significant difference between the 2 groups. In Group 1, the differences of effective rate of Timolol therapy between each of the 2 subgroups of age, gender, preoperative SE (PSE), or pretreatment time (how long we start treatment with Timolol post-LASIK) were not statistically significant.
Conclusion: IOP-lowering eye drop Timolol was effective for the correction of myopic regression when a 0.5-D or greater myopic shift is detected after LASIK in patients regardless of age, gender, PSE, or anytime we started the treatment only if regression happened. However, the myopic regression recurred after cessation of Timolol treatment.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Effect of timolol maleate (0.5%) in the management of myopic regression post laser-assisted in-situ keratomileusis: Clinical and topographical outcomes.Indian J Ophthalmol. 2020 Dec;68(12):2990-2994. doi: 10.4103/ijo.IJO_1503_20. Indian J Ophthalmol. 2020. PMID: 33229683 Free PMC article.
-
Effect of timolol on refractive outcomes in eyes with myopic regression after laser in situ keratomileusis: a prospective randomized clinical trial.Am J Ophthalmol. 2012 Nov;154(5):790-798.e1. doi: 10.1016/j.ajo.2012.05.013. Epub 2012 Aug 28. Am J Ophthalmol. 2012. PMID: 22935601 Clinical Trial.
-
[Preliminary study on preventive effects of timolol on myopic regression after laser in situ keratomileusis].Zhonghua Yan Ke Za Zhi. 2011 Jul;47(7):596-600. Zhonghua Yan Ke Za Zhi. 2011. PMID: 22041483 Clinical Trial. Chinese.
-
Effects of antiglaucoma drugs on refractive outcomes in eyes with myopic regression after laser in situ keratomileusis.Am J Ophthalmol. 2008 Feb;145(2):233-238. doi: 10.1016/j.ajo.2007.09.036. Epub 2007 Dec 11. Am J Ophthalmol. 2008. PMID: 18054889 Clinical Trial.
-
Outcomes of presbyopia-correcting intraocular lenses after laser in situ keratomileusis.Int Ophthalmol. 2019 May;39(5):1199-1204. doi: 10.1007/s10792-018-0908-0. Epub 2018 Mar 28. Int Ophthalmol. 2019. PMID: 29594789 Review.
Cited by
-
Brimonidine tartrate 0.15% drops to reduce low post-LASIK residual myopia: A retrospective study.PLoS One. 2025 Jul 30;20(7):e0329364. doi: 10.1371/journal.pone.0329364. eCollection 2025. PLoS One. 2025. PMID: 40737267 Free PMC article.
-
Effect of timolol maleate (0.5%) in the management of myopic regression post laser-assisted in-situ keratomileusis: Clinical and topographical outcomes.Indian J Ophthalmol. 2020 Dec;68(12):2990-2994. doi: 10.4103/ijo.IJO_1503_20. Indian J Ophthalmol. 2020. PMID: 33229683 Free PMC article.
-
Reduction of corneal epithelial thickness during medical treatment for myopic regression following FS-LASIK.BMC Ophthalmol. 2020 Jul 18;20(1):296. doi: 10.1186/s12886-020-01570-2. BMC Ophthalmol. 2020. PMID: 32682402 Free PMC article.
-
Complications of laser-assisted in situ keratomileusis.Indian J Ophthalmol. 2021 Jul;69(7):1658-1669. doi: 10.4103/ijo.IJO_1872_20. Indian J Ophthalmol. 2021. PMID: 34146007 Free PMC article. Review.
References
-
- Chen YI, Chien KL, Wang IJ, et al. An interval-censored model for predicting myopic regression after laser in situ keratomileusis. Invest Ophthalmol Vis Sci 2007;48:3516–23. - PubMed
-
- Baek T, Lee K, Kagaya F, et al. Factors affecting the forward shift of posterior corneal surface after laser in situ keratomileusis. Ophthalmology 2001;108:317–20. - PubMed
-
- Chayet AS, Assil KK, Montes M, et al. Regression and its mechanisms after laser in situ keratomileusis in moderate and high myopia. Ophthalmology 1998;105:1194–9. - PubMed
-
- Qi H, Hao Y, Xia Y, et al. Regression-related factors before and after laser in situ keratomileusis. Ophthalmologica 2006;220:272–6. - PubMed
-
- Weiss JS, Mokhtarzadeh M. Myopic regression after laser in situ keratomileusis: a medical alternative to surgical enhancement. Am J Ophthalmol 2008;145:189–90. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
