

Tradeoff-in-the-Nephron: A Theory to Explain the Primacy of Phosphate in the Pathogenesis of Secondary Hyperparathyroidism
- PMID: 28445401
- PMCID: PMC5452157
- DOI: 10.3390/nu9050427
Tradeoff-in-the-Nephron: A Theory to Explain the Primacy of Phosphate in the Pathogenesis of Secondary Hyperparathyroidism
Abstract
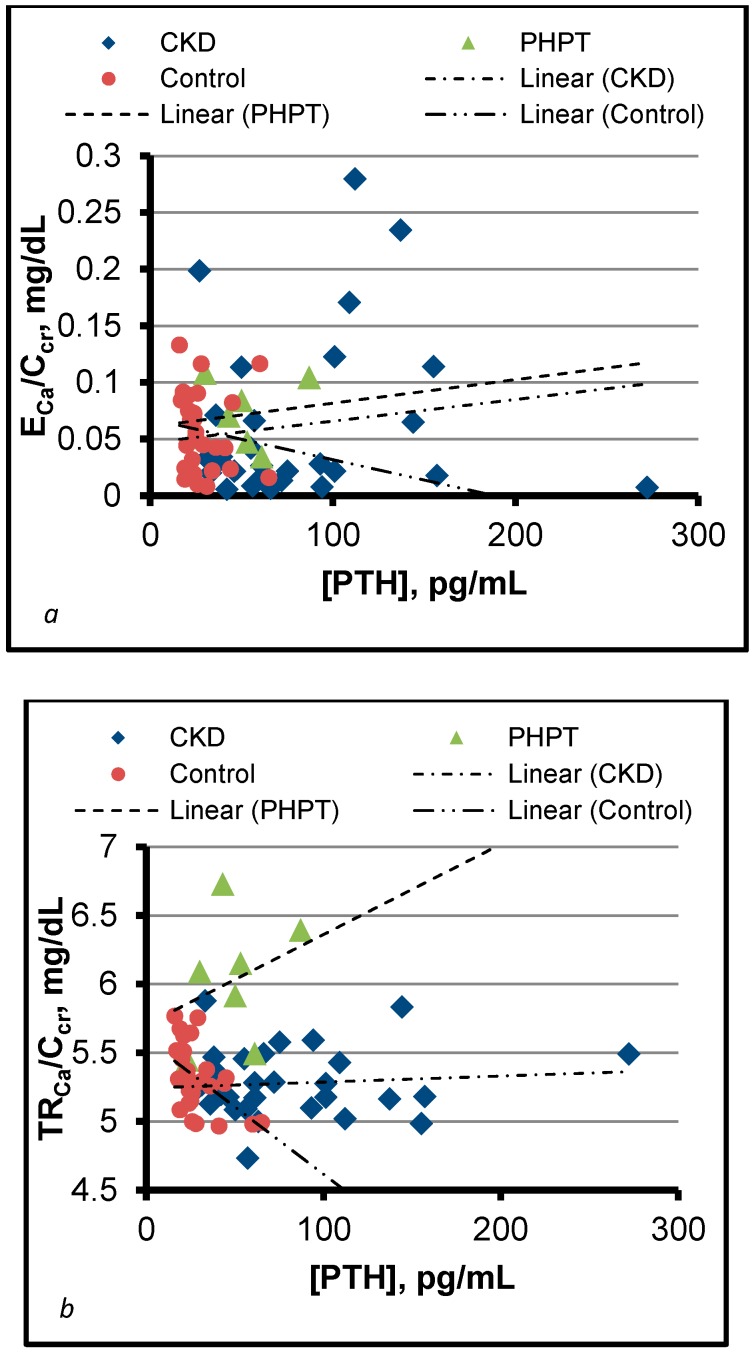
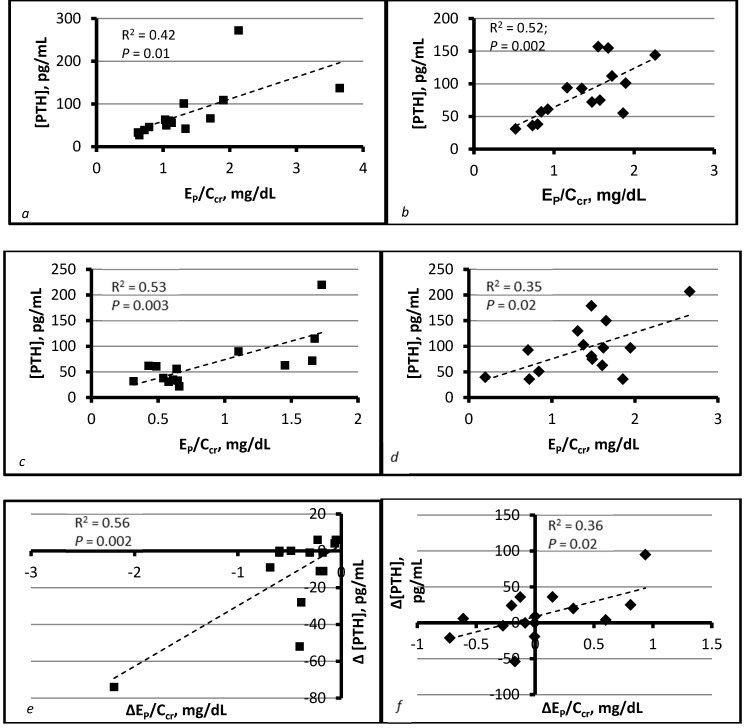
Chronic kidney disease (CKD) causes secondary hyperparathyroidism (SHPT). The cardinal features of SHPT are persistence of normocalcemia as CKD progresses and dependence of the parathyroid hormone concentration ([PTH]) on phosphate influx (IP). The tradeoff-in-the-nephron hypothesis integrates these features. It states that as the glomerular filtration rate (GFR) falls, the phosphate concentration ([P]CDN) rises in the cortical distal nephron, the calcium concentration ([Ca]CDN) in that segment falls, and [PTH] rises to maintain normal calcium reabsorption per volume of filtrate (TRCa/GFR). In a clinical study, we set GFR equal to creatinine clearance (Ccr) and IP equal to the urinary excretion rate of phosphorus (EP). We employed EP/Ccr as a surrogate for [P]CDN. We showed that TRCa/Ccr was high in patients with primary hyperparathyroidism (PHPT) and normal in those with SHPT despite comparably increased [PTH] in each group. In subjects with SHPT, we examined regressions of [PTH] on EP/Ccr before and after treatment with sevelamer carbonate or a placebo. All regressions were significant, and ∆[PTH] correlated with ∆EP/Ccr in each treatment cohort. We concluded that [P]CDN determines [PTH] in CKD. This inference explains the cardinal features of SHPT, much of the evidence on which other pathogenic theories are based, and many ancillary observations.
Keywords: calcium; chronic kidney disease; cortical distal nephron; distal convoluted tubule; parathyroid hormone; phosphate; secondary hyperparathyroidism.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
-
- Levin A., Bakris G.L., Molitch M., Smulders M., Tian J., Williams L.A., Andress D.L. Prevalence of abnormal serum vitamin D, PTH, calcium and phosphorus in patients with chronic kidney disease: Results of the study to evaluate early kidney disease. Kidney Int. 2007;71:31–38. doi: 10.1038/sj.ki.5002009. - DOI - PubMed
-
- Craver L., Marco M.P., Martinez I., Rue M., Borras M., Martin M.L., Sarro F., Valdivielso J.M., Fernandez E. Mineral metabolism parameters throughout chronic kidney disease stages 1–5—Achievement of K/DOQI target ranges. Nephrol. Dial. Transplant. 2007;22:1171–1176. doi: 10.1093/ndt/gfl718. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
