

Cost-effectiveness of a transitional pharmaceutical care program for patients discharged from the hospital
- PMID: 28445474
- PMCID: PMC5406030
- DOI: 10.1371/journal.pone.0174513
Cost-effectiveness of a transitional pharmaceutical care program for patients discharged from the hospital
Abstract
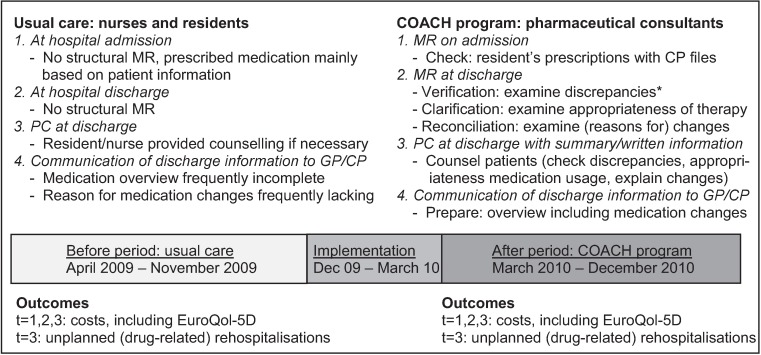
Background: To improve continuity of care at hospital admission and discharge and to decrease medication errors pharmaceutical care programs are developed. This study aims to determine the cost-effectiveness of the COACH program in comparison with usual care from a societal perspective.
Methods: A controlled clinical trial was performed at the Internal Medicine department of a general teaching hospital. All admitted patients using at least one prescription drug were included. The COACH program consisted of medication reconciliation, patient counselling at discharge, and communication to healthcare providers in primary care. The primary outcome was the proportion of patients with an unplanned rehospitalisation within three months after discharge. Also, the number of quality-adjusted life-years (QALYs) was assessed. Cost data were collected using cost diaries. Uncertainty surrounding cost differences and incremental cost-effectiveness ratios between the groups was estimated by bootstrapping.
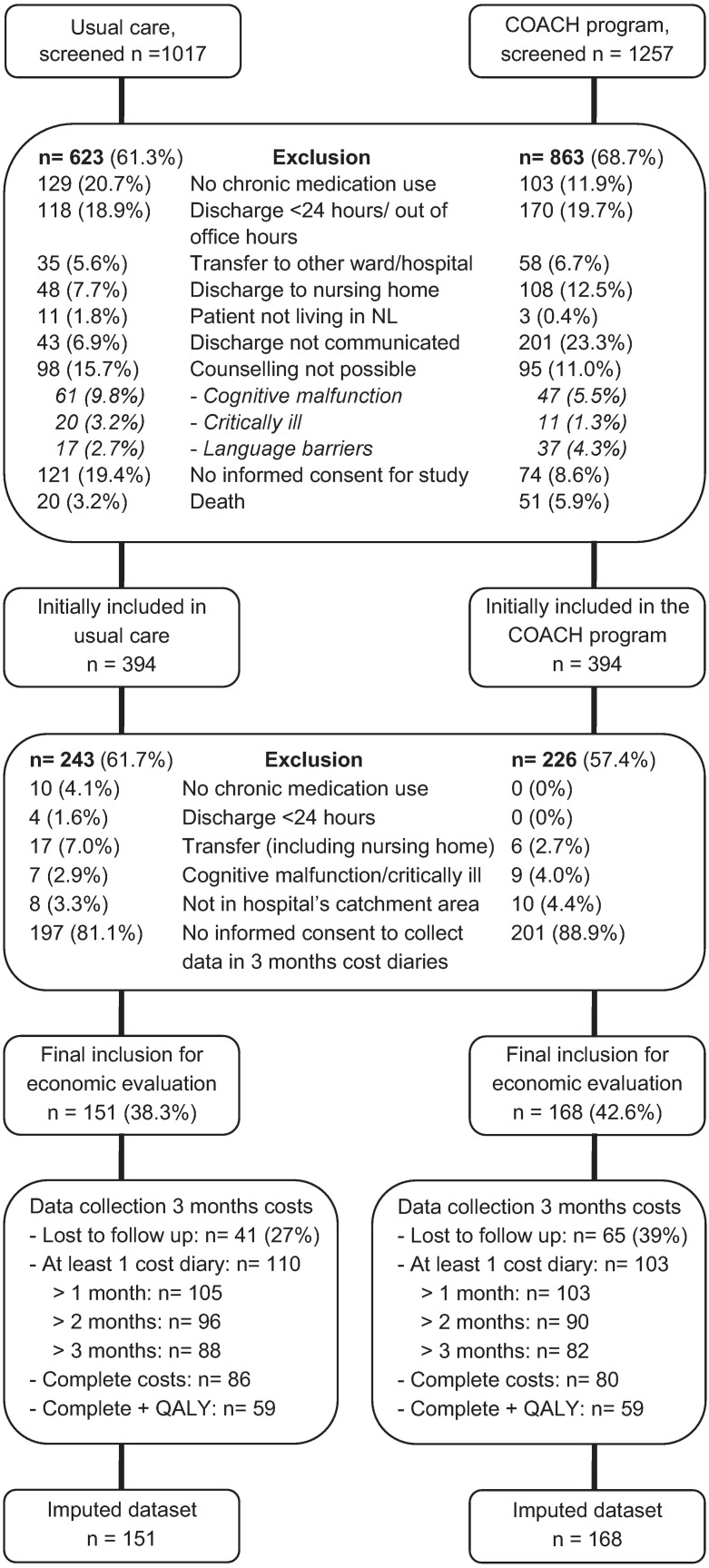
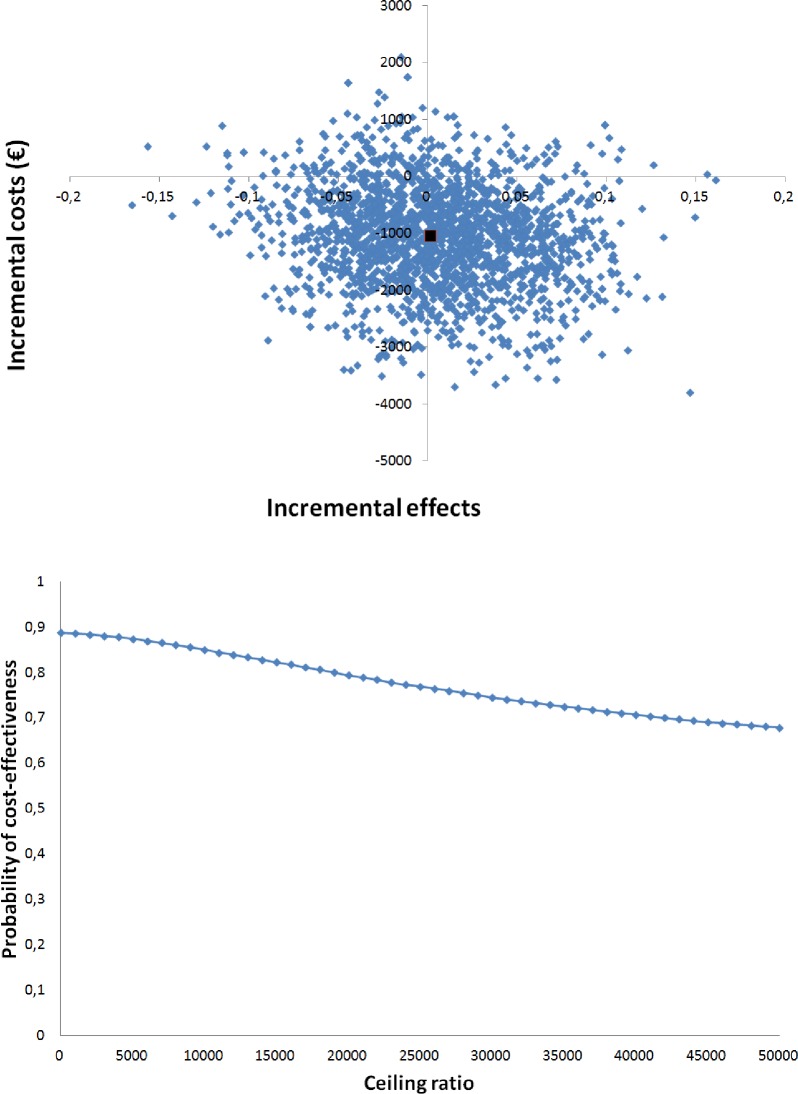
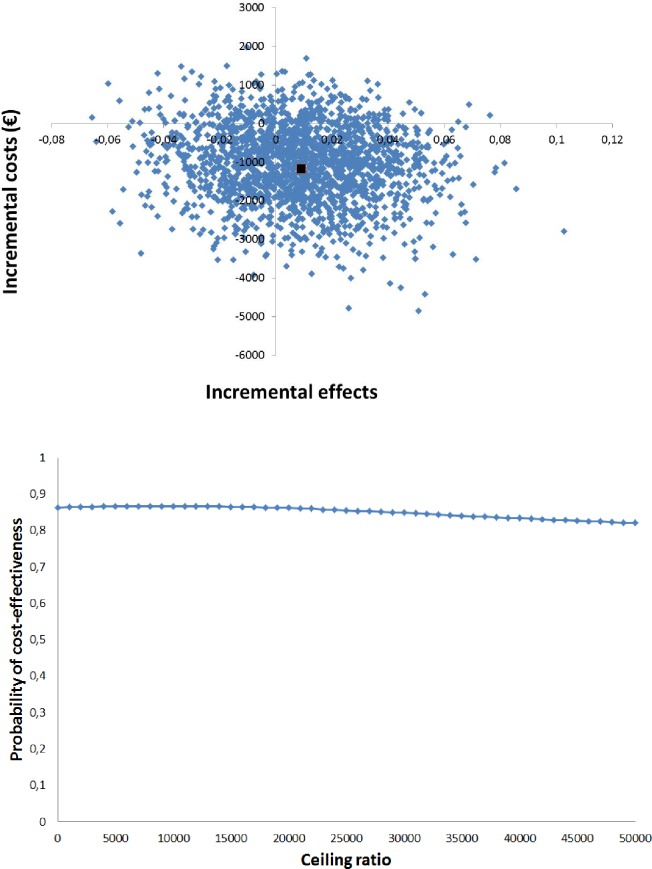
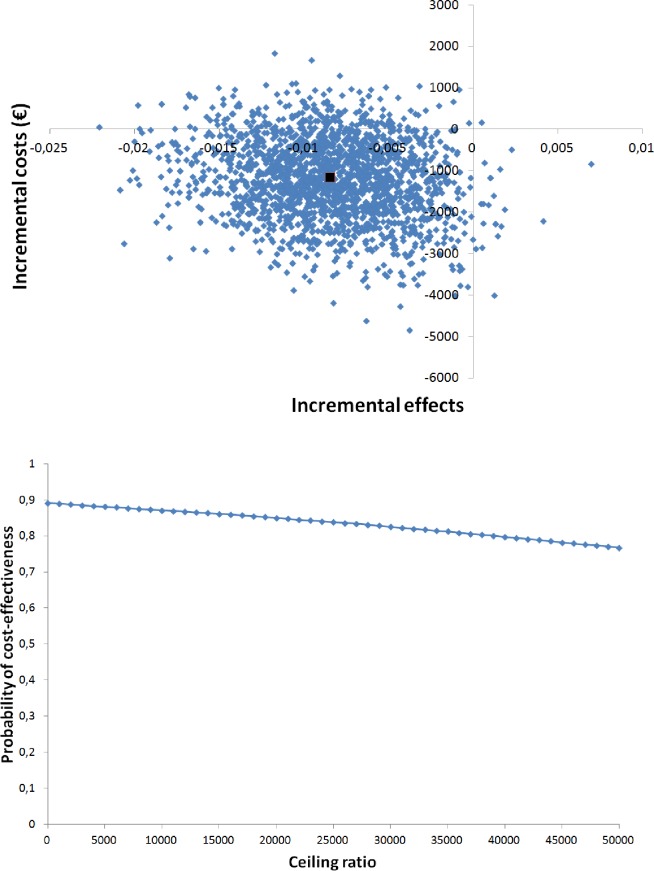
Results: In the COACH program, 168 patients were included and in usual care 151 patients. There was no significant difference in the proportion of patients with unplanned rehospitalisations (mean difference 0.17%, 95% CI -8.85;8.51), and in QALYs (mean difference -0.0085, 95% CI -0.0170;0.0001). Total costs for the COACH program were non-significantly lower than usual care (-€1160, 95% CI -3168;847). Cost-effectiveness planes showed that the program was not cost-effective compared with usual care for unplanned rehospitalisations and QALYs gained.
Conclusion: The COACH program was not cost-effective in comparison with usual care. Future studies should focus on high risk patients and include other outcomes (e.g. adverse drug events) as this may increase the chances of a cost-effective intervention. Dutch trial register NTR1519.
Conflict of interest statement
Figures
References
-
- Parry C, Coleman EA, Smith JD, Frank J, Kramer AM. The care transitions intervention: a patient-centered approach to ensuring effective transfers between sites of geriatric care. Home Health Care Serv Q. 2003;22(3): 1–17. doi: 10.1300/J027v22n03_01 - DOI - PubMed
-
- Coleman EA, Smith JD, Raha D, Min SJ. Posthospital medication discrepancies: prevalence and contributing factors. Arch Intern Med. 2005;165(16): 1842–1847. doi: 10.1001/archinte.165.16.1842 - DOI - PubMed
-
- Cornish PL, Knowles SR, Marchesano R, Tam V, Shadowitz S, Juurlink DN, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4): 424–429. doi: 10.1001/archinte.165.4.424 - DOI - PubMed
-
- Vira T, Colquhoun M, Etchells E. Reconcilable differences: correcting medication errors at hospital admission and discharge. Qual Saf Health Care. 2006;15(2): 122–126. doi: 10.1136/qshc.2005.015347 - DOI - PMC - PubMed
-
- Karapinar-Carkit F, Borgsteede SD, Zoer J, Smit HJ, Egberts AC, van den Bemt PM. Effect of medication reconciliation with and without patient counseling on the number of pharmaceutical interventions among patients discharged from the hospital. Ann Pharmacother. 2009;43(6): 1001–1010. doi: 10.1345/aph.1L597 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
