

Sensitivity and Specificity of Cetuximab-IRDye800CW to Identify Regional Metastatic Disease in Head and Neck Cancer
- PMID: 28446503
- PMCID: PMC5595145
- DOI: 10.1158/1078-0432.CCR-16-2968
Sensitivity and Specificity of Cetuximab-IRDye800CW to Identify Regional Metastatic Disease in Head and Neck Cancer
Abstract
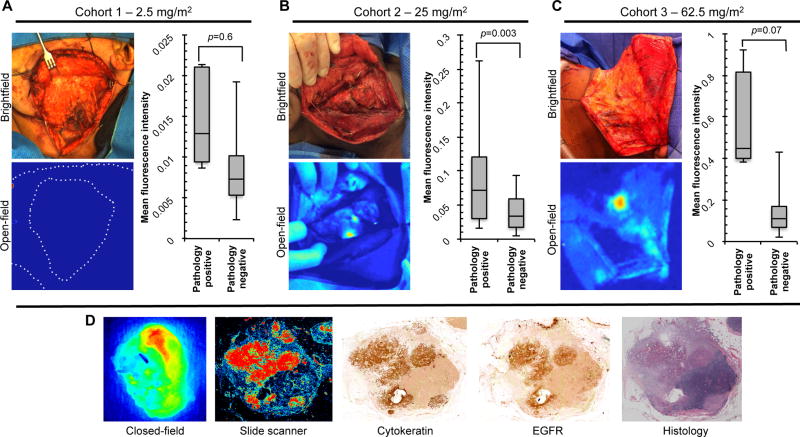
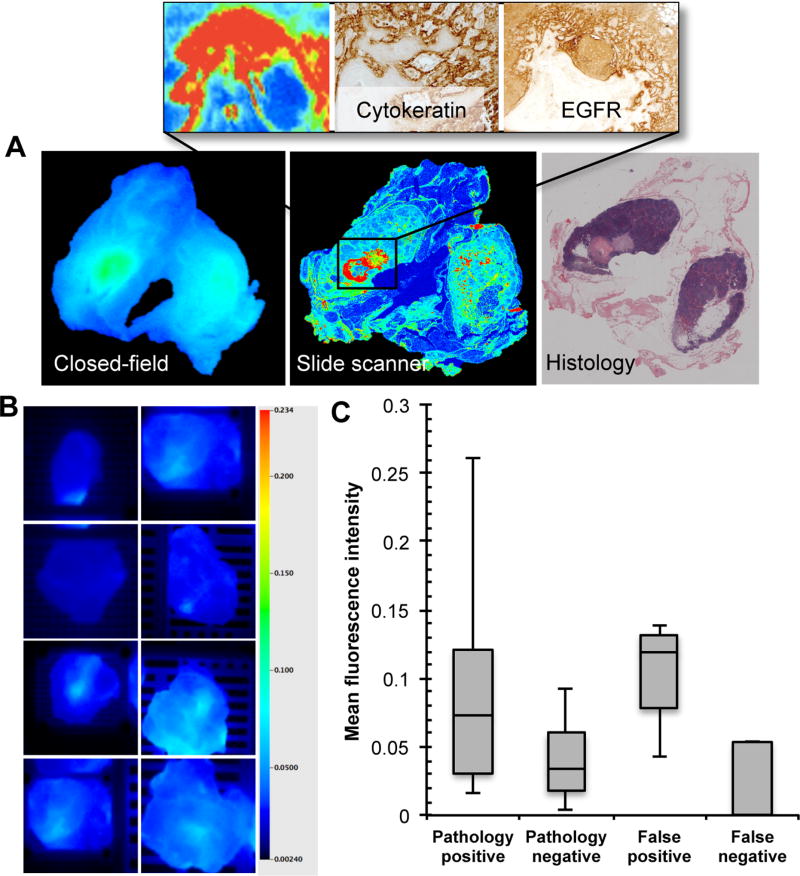
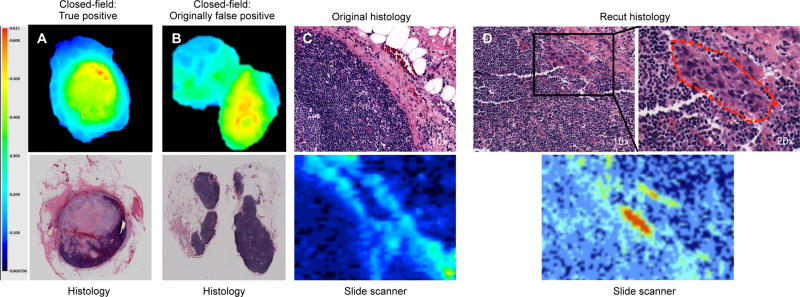
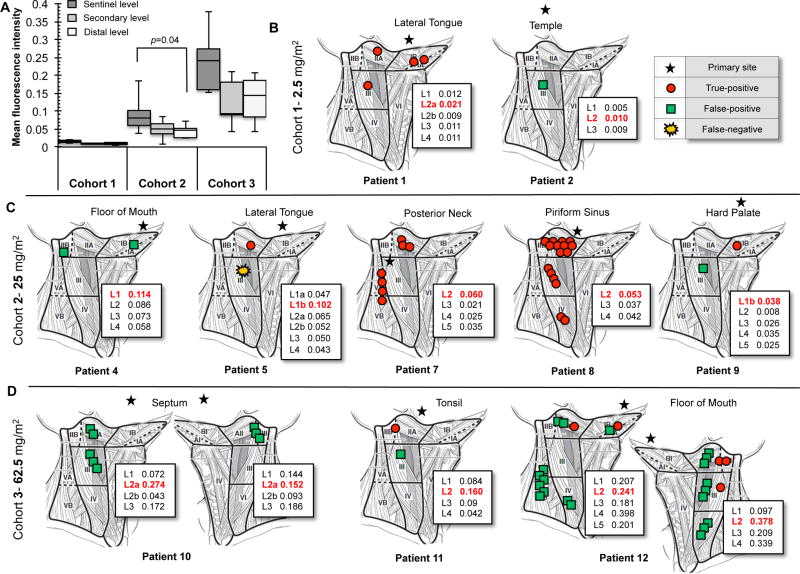
Purpose: Comprehensive cervical lymphadenectomy can be associated with significant morbidity and poor quality of life. This study evaluated the sensitivity and specificity of cetuximab-IRDye800CW to identify metastatic disease in patients with head and neck cancer.Experimental Design: Consenting patients scheduled for curative resection were enrolled in a clinical trial to evaluate the safety and specificity of cetuximab-IRDye800CW. Patients (n = 12) received escalating doses of the study drug. Where indicated, cervical lymphadenectomy accompanied primary tumor resection, which occurred 3 to 7 days following intravenous infusion of cetuximab-IRDye800CW. All 471 dissected lymph nodes were imaged with a closed-field, near-infrared imaging device during gross processing of the fresh specimens. Intraoperative imaging of exposed neck levels was performed with an open-field fluorescence imaging device. Blinded assessments of the fluorescence data were compared to histopathology to calculate sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV).Results: Of the 35 nodes diagnosed pathologically positive, 34 were correctly identified with fluorescence imaging, yielding a sensitivity of 97.2%. Of the 435 pathologically negative nodes, 401 were correctly assessed using fluorescence imaging, yielding a specificity of 92.7%. The NPV was determined to be 99.7%, and the PPV was 50.7%. When 37 fluorescently false-positive nodes were sectioned deeper (1 mm) into their respective blocks, metastatic cancer was found in 8.1% of the recut nodal specimens, which altered staging in two of those cases.Conclusions: Fluorescence imaging of lymph nodes after systemic cetuximab-IRDye800CW administration demonstrated high sensitivity and was capable of identifying additional positive nodes on deep sectioning. Clin Cancer Res; 23(16); 4744-52. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures
References
-
- Arbes SJ, Jr, Olshan AF, Caplan DJ, Schoenbach VJ, Slade GD, Symons MJ. Factors contributing to the poorer survival of black Americans diagnosed with oral cancer (United States) Cancer causes & control : CCC. 1999;10:513–23. - PubMed
-
- Ozdek A, Sarac S, Akyol MU, Unal OF, Sungur A. Histopathological predictors of occult lymph node metastases in supraglottic squamous cell carcinomas. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies. 2000;257:389–92. - PubMed
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA: a cancer journal for clinicians. 2008;58:71–96. - PubMed
-
- Leong SP, Cady B, Jablons DM, Garcia-Aguilar J, Reintgen D, Jakub J, et al. Clinical patterns of metastasis. Cancer metastasis reviews. 2006;25:221–32. - PubMed
-
- Howell GM, Grandis JR. Molecular mediators of metastasis in head and neck squamous cell carcinoma. Head & neck. 2005;27:710–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
