

Donor-Specific Antibodies in Kidney Transplant Recipients
- PMID: 28446536
- PMCID: PMC5753302
- DOI: 10.2215/CJN.00700117
Donor-Specific Antibodies in Kidney Transplant Recipients
Abstract
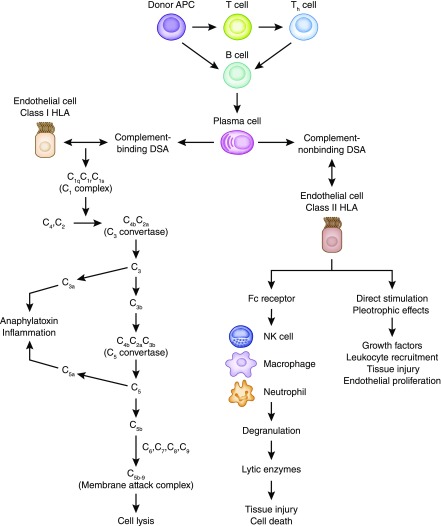
Donor-specific antibodies have become an established biomarker predicting antibody-mediated rejection. Antibody-mediated rejection is the leading cause of graft loss after kidney transplant. There are several phenotypes of antibody-mediated rejection along post-transplant course that are determined by the timing and extent of humoral response and the various characteristics of donor-specific antibodies, such as antigen classes, specificity, antibody strength, IgG subclasses, and complement binding capacity. Preformed donor-specific antibodies in sensitized patients can trigger hyperacute rejection, accelerated acute rejection, and early acute antibody-mediated rejection. De novo donor-specific antibodies are associated with late acute antibody-mediated rejection, chronic antibody-mediated rejection, and transplant glomerulopathy. The pathogeneses of antibody-mediated rejection include not only complement-dependent cytotoxicity, but also complement-independent pathways of antibody-mediated cellular cytotoxicity and direct endothelial activation and proliferation. The novel assay for complement binding capacity has improved our ability to predict antibody-mediated rejection phenotypes. C1q binding donor-specific antibodies are closely associated with acute antibody-mediated rejection, more severe graft injuries, and early graft failure, whereas C1q nonbinding donor-specific antibodies correlate with subclinical or chronic antibody-mediated rejection and late graft loss. IgG subclasses have various abilities to activate complement and recruit effector cells through the Fc receptor. Complement binding IgG3 donor-specific antibodies are frequently associated with acute antibody-mediated rejection and severe graft injury, whereas noncomplement binding IgG4 donor-specific antibodies are more correlated with subclinical or chronic antibody-mediated rejection and transplant glomerulopathy. Our in-depth knowledge of complex characteristics of donor-specific antibodies can stratify the patient's immunologic risk, can predict distinct phenotypes of antibody-mediated rejection, and hopefully, will guide our clinical practice to improve the transplant outcomes.
Keywords: Biomarkers; C1q-binding DSA; Complement System Proteins; Humans; IgG subclasses; Immunoglobulin G; Phenotype; Receptors, Fc; Tissue Donors; antibody-mediated rejection; donor specific antibody; kidney transplantation.
Copyright © 2018 by the American Society of Nephrology.
Figures
References
-
- Halloran PF, Reeve JP, Pereira AB, Hidalgo LG, Famulski KS: Antibody-mediated rejection, T cell-mediated rejection, and the injury-repair response: New insights from the Genome Canada studies of kidney transplant biopsies. Kidney Int 85: 258–264, 2014 - PubMed
-
- Sellarés J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF: Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12: 388–399, 2012 - PubMed
-
- Lawrence C, Willicombe M, Brookes PA, Santos-Nunez E, Bajaj R, Cook T, Roufosse C, Taube D, Warrens AN: Preformed complement-activating low-level donor-specific antibody predicts early antibody-mediated rejection in renal allografts. Transplantation 95: 341–346, 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
