

Zenker's diverticulum: flexible versus rigid repair
- PMID: 28446979
- PMCID: PMC5384898
- DOI: 10.21037/jtd.2017.03.133
Zenker's diverticulum: flexible versus rigid repair
Abstract
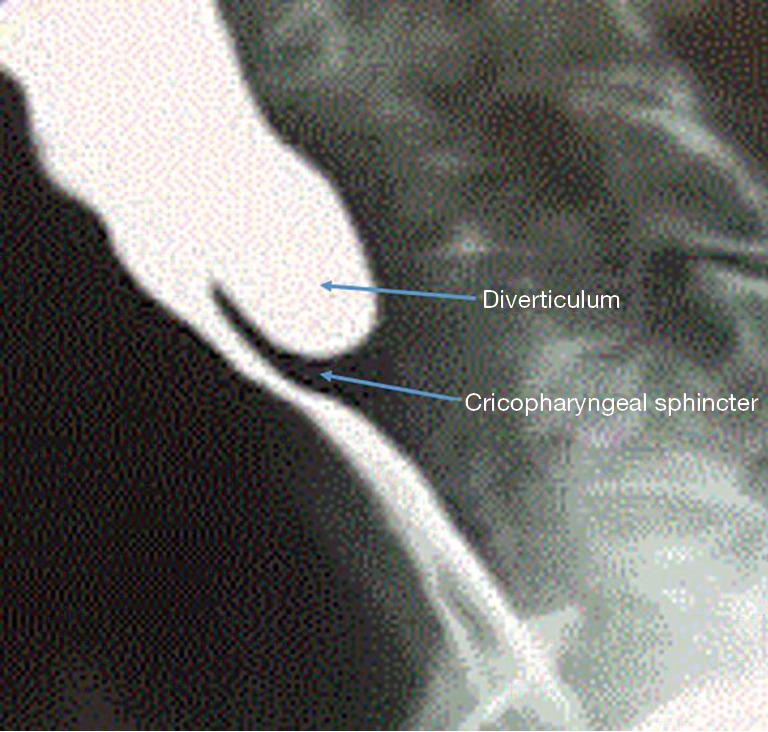
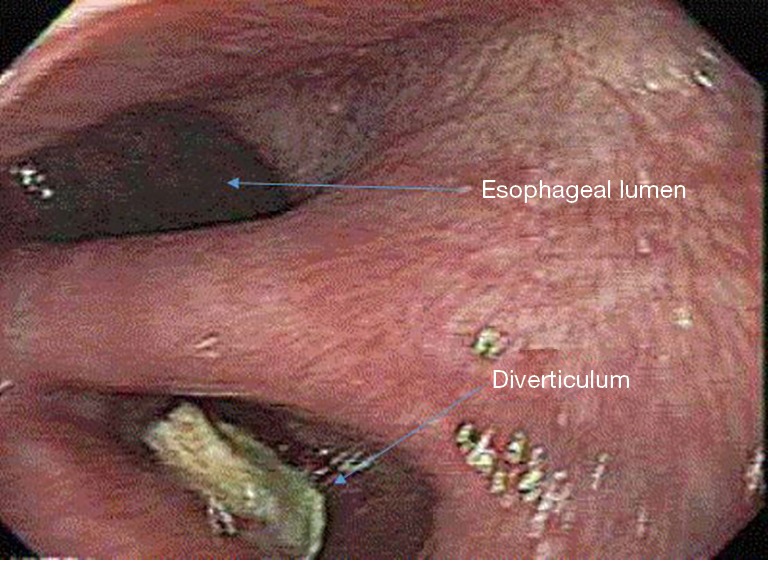
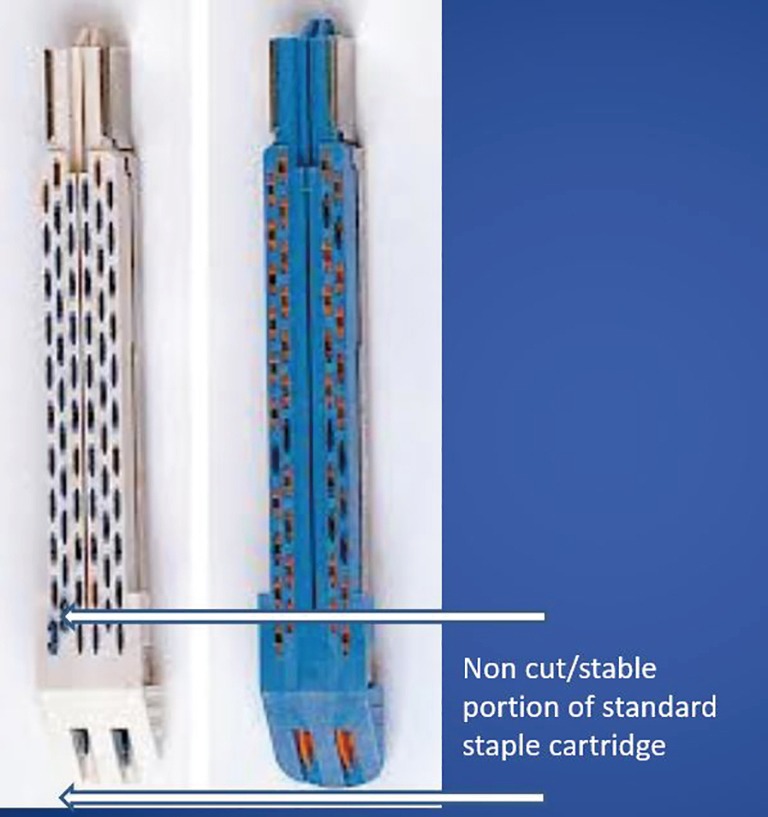
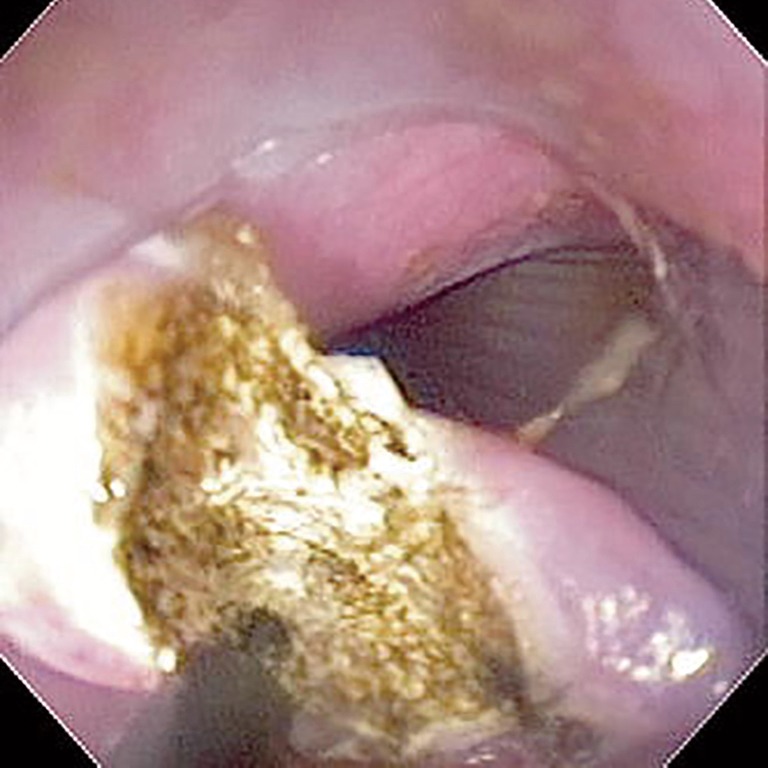
Zenker's diverticula (ZDs) are a relatively common cause of cervical dysphagia. Diagnosis is best by a good upper GI exam though upper endoscopy should be performed as well. Treatment is either by open, transcervical approaches or trans-oral. Over the past 20 years, transoral approach has mostly replace transcervical approaches due to less pain, no scarring and a rapid recovery. Transoral approaches are either using rigid access or flexible endoscopy. Today, the most common approach is transoral stapling using a 12 mm laparoscopic linear cutting stapler. This has the drawbacks of requiring extreme neck extension, the massive size of the stapler making visualization mostly impossible and the current staple design that does not cut/staple all the way to the end of the blades-resulting in a residual pouch. Flexible endoscopy allows a more tailored approach under direct vision, the myotomy can even be extended beyond the diverticulum and onto the esophageal wall to minimize the risk of incomplete myotomy. Experienced endoscopists report high technical success and low complication. Success rates are similar but maybe slightly higher than with ridged transoral approaches or open surgery. Today, flexible endoscopic Zenkers is our preferred initial approach-with open or ridged being reserved for special indications.
Keywords: Zenkers; cricopharyngeal; diverticulum; endoscopy; myotomy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous