

Alternative conduits for esophageal replacement
- PMID: 28447002
- PMCID: PMC5387143
- DOI: 10.21037/acs.2017.03.07
Alternative conduits for esophageal replacement
Abstract
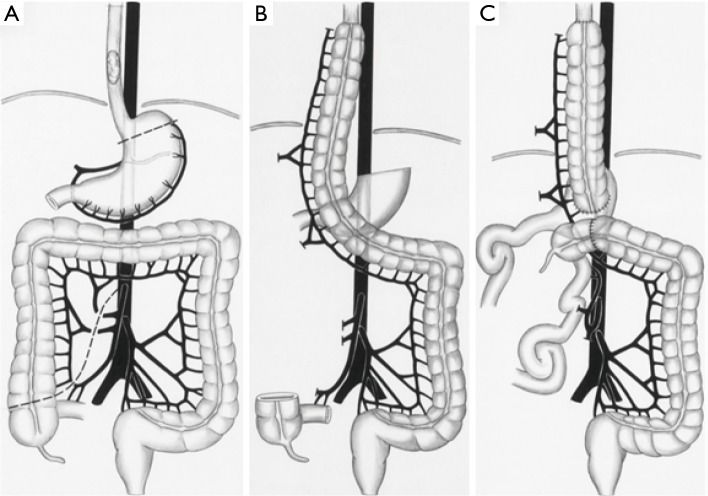
Replacement of the native esophagus after esophagectomy is a problem that has challenged surgeons for over a century. Not only must the conduit be long enough to bridge the distance between the cervical esophagus and the abdomen, it must also have a reliable vascular supply and be sufficiently functional to allow for deglutition. The stomach, jejunum, and colon (right, left or transverse) have all been proposed as potential solutions. The stomach has gained favor for its length, reliable vascular supply and need for only a single anastomosis. However, there are times when the stomach is unavailable for use as a conduit. It is in these instances that an esophageal surgeon must have an alternative conduit in their armamentarium. In this paper, we will briefly discuss the technical aspects of jejunal and colonic interposition. We will review the recent literature with a focus on early and late outcomes. The advantages and disadvantages of both options will be reviewed.
Keywords: Esophagectomy; Roux-en-Y jejunostomy; colon interposition; esophageal; jejunum.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- DeMeester SR. Colonic Interposition for Benign Disease. Oper Tech Thorac Cardiovasc Surg 2006;11:232-49. 10.1053/j.optechstcvs.2006.08.003 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials