

Validity of the Montreal Cognitive Assessment Screener in Adolescents and Young Adults With and Without Congenital Heart Disease
- PMID: 28448372
- PMCID: PMC5408464
- DOI: 10.1097/NNR.0000000000000192
Validity of the Montreal Cognitive Assessment Screener in Adolescents and Young Adults With and Without Congenital Heart Disease
Abstract
Background: Cognitive deficits are common, long-term sequelae in children and adolescents with congenital heart disease (CHD) who have undergone surgical palliation. However, there is a lack of a validated brief cognitive screening tool appropriate for the outpatient setting for adolescents with CHD. One candidate instrument is the Montreal Cognitive Assessment (MoCA) questionnaire.
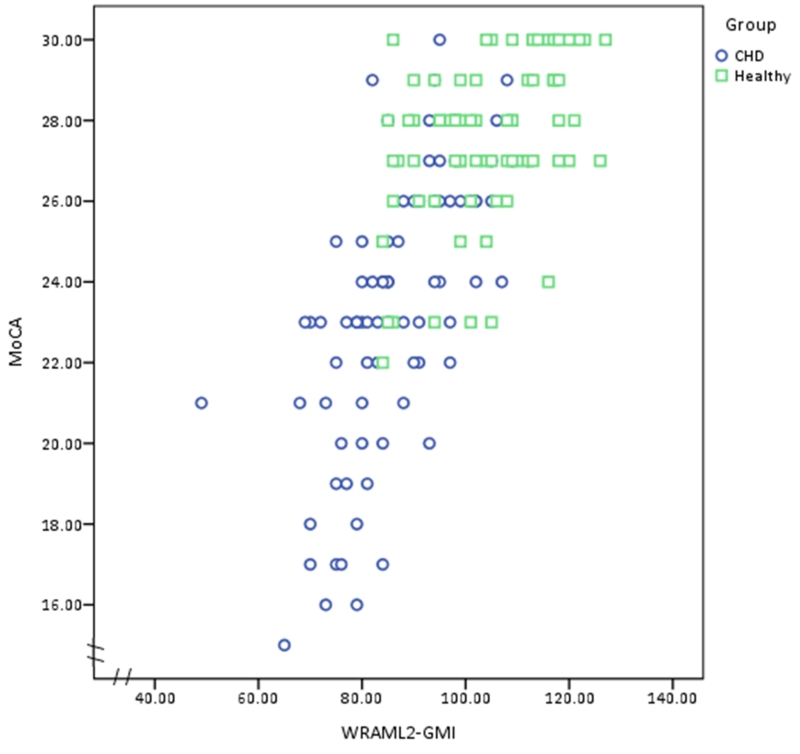
Objective: The purpose of the research was to validate scores from the MoCA against the General Memory Index (GMI) of the Wide Range Assessment of Memory and Learning, 2nd Edition (WRAML2), a widely accepted measure of cognition/memory, in adolescents and young adults with CHD.
Methods: We administered the MoCA and the WRAML2 to 156 adolescents and young adults ages 14-21 (80 youth with CHD and 76 healthy controls who were gender and age matched). Spearman's rank order correlations were used to assess concurrent validity. To assess construct validity, the Mann-Whitney U test was used to compare differences in scores in youth with CHD and the healthy control group. Receiver operating characteristic curves were created and area under the curve, sensitivity, specificity, positive predictive value, and negative predictive value were also calculated.
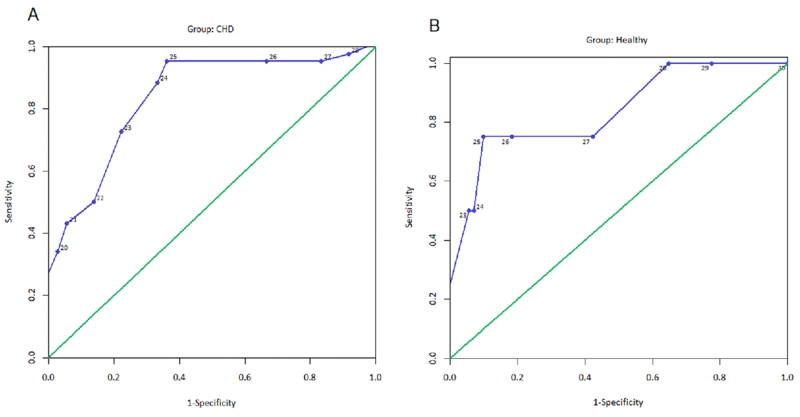
Results: The MoCA median scores in the CHD versus healthy controls were (23, range 15-29 vs. 28, range 22-30; p < .001), respectively. With the screening cutoff scores at <26 points for the MoCA and 85 for GMI (<1 SD, M = 100, SD = 15), the CHD versus healthy control groups showed sensitivity of .96 and specificity of .67 versus sensitivity of .75 and specificity of .90, respectively, in the detection of cognitive deficits. A cutoff score of 26 on the MoCA was optimal in the CHD group; a cutoff of 25 had similar properties except for a lower negative predictive value. The area under the receiver operating characteristic curve (95% CI) for the MoCA was 0.84 (95% CI [0.75, 0.93], p < .001) and 0.84 (95% CI [0.62, 1.00], p = .02) for the CHD and controls, respectively.
Discussion: Scores on the MoCA were valid for screening to detect cognitive deficits in adolescents and young adults aged 14-21 with CHD when a cutoff score of 26 is used to differentiate youth with and without significant cognitive impairment. Future studies are needed in other adolescent disease groups with known cognitive deficits and healthy populations to explore the generalizability of validity of MoCA scores in adolescents and young adults.
Figures
Similar articles
-
Is the Montreal Cognitive Assessment superior to the Mini-Mental State Examination to detect poststroke cognitive impairment? A study with neuropsychological evaluation.Stroke. 2011 Jun;42(6):1712-6. doi: 10.1161/STROKEAHA.110.606277. Epub 2011 Apr 7. Stroke. 2011. PMID: 21474808
-
Validation of the Turkish Version of the Montreal Cognitive Assessment Scale (MoCA-TR) in patients with Parkinson's disease.Clin Neuropsychol. 2014;28(2):333-43. doi: 10.1080/13854046.2014.881554. Epub 2014 Feb 17. Clin Neuropsychol. 2014. PMID: 24528299
-
Validity of the Cantonese Chinese Montreal Cognitive Assessment in Southern Chinese.Geriatr Gerontol Int. 2015 Jan;15(1):96-103. doi: 10.1111/ggi.12237. Epub 2014 Jan 24. Geriatr Gerontol Int. 2015. PMID: 24456109
-
A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores.Int J Geriatr Psychiatry. 2018 Feb;33(2):379-388. doi: 10.1002/gps.4756. Epub 2017 Jul 21. Int J Geriatr Psychiatry. 2018. PMID: 28731508
-
Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis.Psychiatr Pol. 2016 Oct 31;50(5):1039-1052. doi: 10.12740/PP/45368. Psychiatr Pol. 2016. PMID: 27992895 Review. English, Polish.
Cited by
-
Clinical Reasoning: A 17-Year-Old Girl With Progressive Cognitive Impairment.Neurology. 2023 Oct 3;101(14):e1466-e1472. doi: 10.1212/WNL.0000000000207597. Epub 2023 Jul 25. Neurology. 2023. PMID: 37491326 Free PMC article.
-
Exploring the Implementation of Cognitive Screening in First-Episode Psychosis Settings: The CogScreen Implementation Study.Early Interv Psychiatry. 2025 Feb;19(2):e70004. doi: 10.1111/eip.70004. Early Interv Psychiatry. 2025. PMID: 39865466 Free PMC article.
-
Cardiovascular and Stroke Nursing Council Science in Review.J Am Heart Assoc. 2019 Apr 2;8(7):e012522. doi: 10.1161/JAHA.119.012522. J Am Heart Assoc. 2019. PMID: 30922160 Free PMC article. No abstract available.
-
Montreal Cognitive Assessment (MoCA) as a screening tool for cognitive impairment in early stages of psychosis.Schizophr Res Cogn. 2024 Jan 29;36:100302. doi: 10.1016/j.scog.2024.100302. eCollection 2024 Jun. Schizophr Res Cogn. 2024. PMID: 38323136 Free PMC article.
-
Reduced brain mammillary body volumes and memory deficits in adolescents who have undergone the Fontan procedure.Pediatr Res. 2020 Jan;87(1):169-175. doi: 10.1038/s41390-019-0569-3. Epub 2019 Sep 9. Pediatr Res. 2020. PMID: 31499515 Free PMC article.
References
-
- Ballweg JA, Wernovsky G, Gaynor JW. Neurodevelopmental outcomes following congenital heart surgery. Pediatric Cardiology. 2007;28:126–133. doi:10.1007/s00246-006-1450-9. - PubMed
-
- Bellinger DC, Wypij D, Rivkin MJ, DeMaso DR, Robertson RL, Dunbar-Masterson C, Newburger JW. Adolescents with d-transposition of the great arteries corrected with the arterial switch procedure: Neuropsychological assessment and structural brain imaging. Circulation. 2011;124:1361–1369. doi:10.1161/CIRCULATIONAHA.111.026963. - PMC - PubMed
-
- Bezdicek O, Majerova V, Novak M, Nikolai T, Ruzicka E, Roth J. Validity of the Montreal Cognitive Assessment in the detection of cognitive dysfunction in Huntington’s disease. Applied Neuropsychology: Adult. 2013;20:33–40. doi:10.1080/09084282.2012.670158. - PubMed
-
- Bornholt LJ, Ajersch S, Fisher IH, Markham RH, Ouvier RA. Cognitive screening for children and adolescents: General limits or ceiling effects? Journal of Child Neurology. 2010;25:567–571. doi:10.1177/0883073809352686. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
