

Left Atrium Measurements via Computed Tomography Pulmonary Angiogram as a Predictor of Diastolic Dysfunction
- PMID: 28448402
- PMCID: PMC5600630
- DOI: 10.1097/RCT.0000000000000597
Left Atrium Measurements via Computed Tomography Pulmonary Angiogram as a Predictor of Diastolic Dysfunction
Abstract
Purpose: Left atrium (LA) enlargement on echocardiography may be an indicator of diastolic dysfunction (DD). It is not well known if computed tomography pulmonary angiography (CTPA) can detect DD.
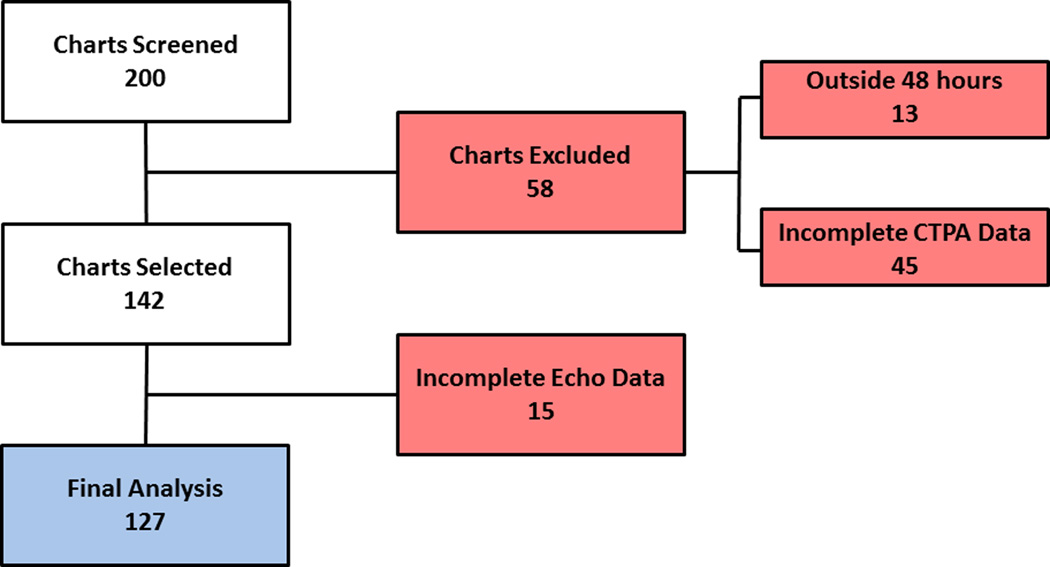
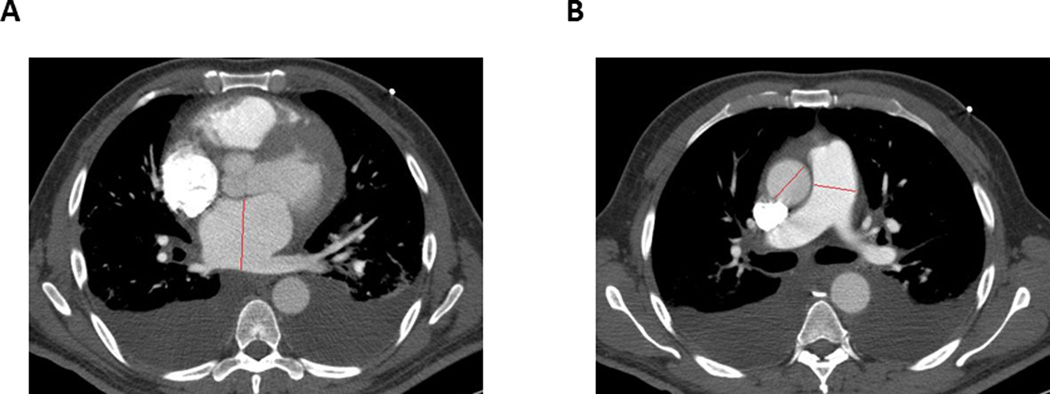
Methods: A total of 127 patients who underwent both CTPA and echo within 48 hours were analyzed retrospectively. Left atrium diameters from CTPA were correlated with echo and evaluated against degrees of DD. Computed tomography pulmonary angiography pulmonary artery (PA)/aorta ratio was analyzed as a tool to detect pulmonary hypertension.
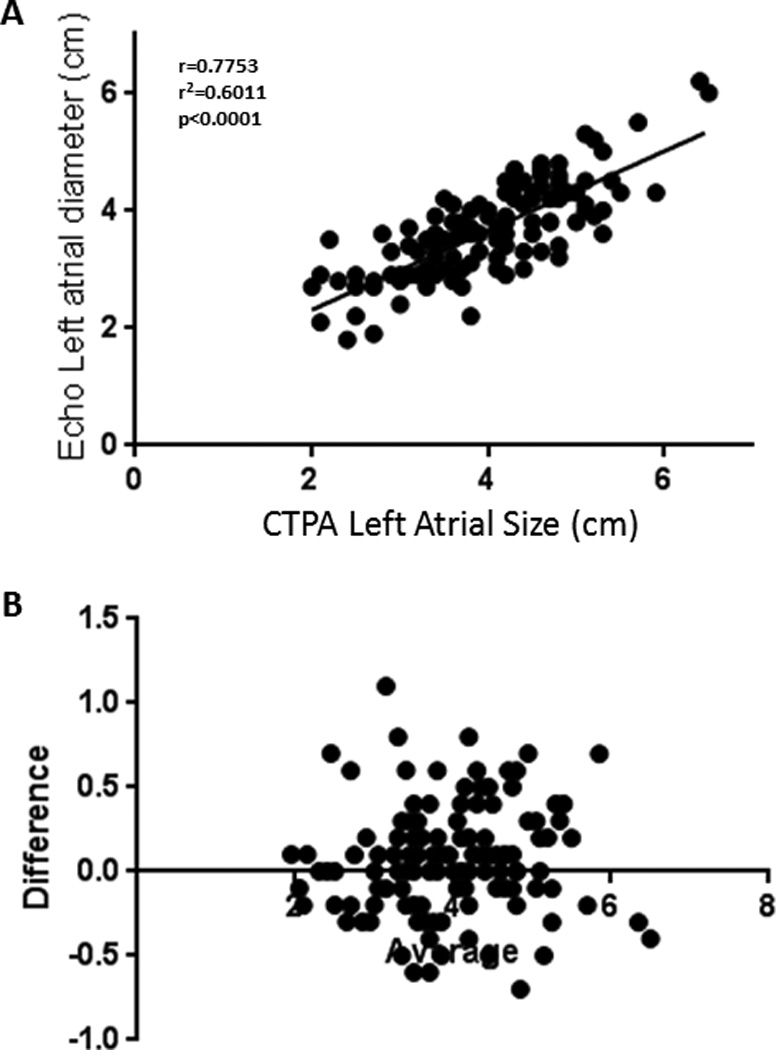
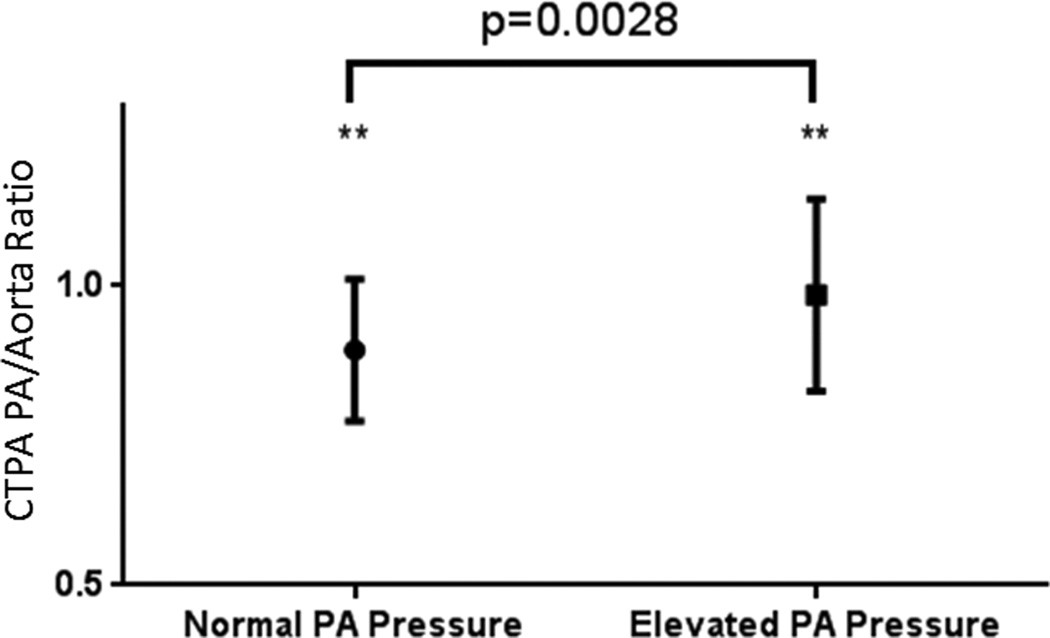
Results: There were 42% of patients who had DD. There was a strong correlation between LA size on CTPA and echo (r = 0.78). An LA greater than 4.0 cm gave a sensitivity of 68.1% and specificity of 73.9% for DD detection. A PA/aorta cutoff greater than 0.84 yielded a sensitivity of 84% and specificity of 33% for pulmonary hypertension.
Conclusions: Computed tomography pulmonary angiography measurements of LA and PA/aorta ratio correlate strongly with equivalent findings on echo. We suggest that LA and PA/aorta measurements be included on chest CTPA reports.
Conflict of interest statement
Figures

Similar articles
-
Utility of Automated Cardiac Chamber Volumetry by Nongated CT Pulmonary Angiography for Detection of Pulmonary Hypertension Using the 2018 Updated Hemodynamic Definition.AJR Am J Roentgenol. 2022 Jul;219(1):66-75. doi: 10.2214/AJR.21.27147. Epub 2022 Jan 26. AJR Am J Roentgenol. 2022. PMID: 35080457
-
Detection of severe pulmonary hypertension based on computed tomography pulmonary angiography.Int J Cardiovasc Imaging. 2021 Aug;37(8):2577-2588. doi: 10.1007/s10554-021-02231-1. Epub 2021 Apr 7. Int J Cardiovasc Imaging. 2021. PMID: 33826018
-
Computed Tomography Pulmonary Angiogram Dynamic Parameter Correlation With Pulmonary Pressure and Pulmonary Hypertension Etiologies.J Comput Assist Tomogr. 2017 Sep/Oct;41(5):779-783. doi: 10.1097/RCT.0000000000000582. J Comput Assist Tomogr. 2017. PMID: 28240636
-
CT derived left atrial size identifies left heart disease in suspected pulmonary hypertension: Derivation and validation of predictive thresholds.Int J Cardiol. 2018 Jun 1;260:172-177. doi: 10.1016/j.ijcard.2018.02.114. Epub 2018 Mar 4. Int J Cardiol. 2018. PMID: 29530618 Free PMC article.
-
Left atrial size measured on CT pulmonary angiography: another parameter of pulmonary embolism severity? A systematic review.J Thromb Thrombolysis. 2020 Jul;50(1):181-189. doi: 10.1007/s11239-019-01994-8. J Thromb Thrombolysis. 2020. PMID: 31754905
Cited by
-
Biatrial Volumetric Assessment by Non-ECG-Gated CT Pulmonary Angiography Correlated with Transthoracic Echocardiography in Patients with Normal Diastology.Tomography. 2022 Nov 17;8(6):2761-2771. doi: 10.3390/tomography8060230. Tomography. 2022. PMID: 36412689 Free PMC article.
-
Isolated Left Atrium Morphofunctional Study of an Experimental Pulmonary Hypertension Model in Rats.Arq Bras Cardiol. 2023 Sep;120(10):e20230188. doi: 10.36660/abc.20230188. Arq Bras Cardiol. 2023. PMID: 37878960 Free PMC article. English, Portuguese.
-
Can left atrial diameter measured by computed tomography predict the presence and degree of left ventricular diastolic dysfunction?Clin Exp Emerg Med. 2024 Dec;11(4):358-364. doi: 10.15441/ceem.24.194. Epub 2024 May 23. Clin Exp Emerg Med. 2024. PMID: 38778493 Free PMC article.
-
The effect of icosapent ethyl on left atrial and left ventricular morphology.Br J Cardiol. 2023 Jul 11;30(3):22. doi: 10.5837/bjc.2023.022. eCollection 2023. Br J Cardiol. 2023. PMID: 39144091 Free PMC article.
References
-
- Zile MR, Baicu CF, Bonnema DD. Diastolic heart failure: definitions and terminology. Prog Cardiovasc Dis. 2005;47:307–313. - PubMed
-
- Liao L, Jollis JG, Anstrom KJ, et al. Costs for heart failure with normal vs reduced ejection fraction. Arch Intern Med. 2006;166:112–118. - PubMed
-
- Tsutsui H, Tsuchihashi M, Takeshita A. Mortality and readmission of hospitalized patients with congestive heart failure and preserved versus depressed systolic function. Am J Cardiol. 2001;88:530–533. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
