

Integrin β1 activation induces an anti-melanoma host response
- PMID: 28448494
- PMCID: PMC5407755
- DOI: 10.1371/journal.pone.0175300
Integrin β1 activation induces an anti-melanoma host response
Abstract
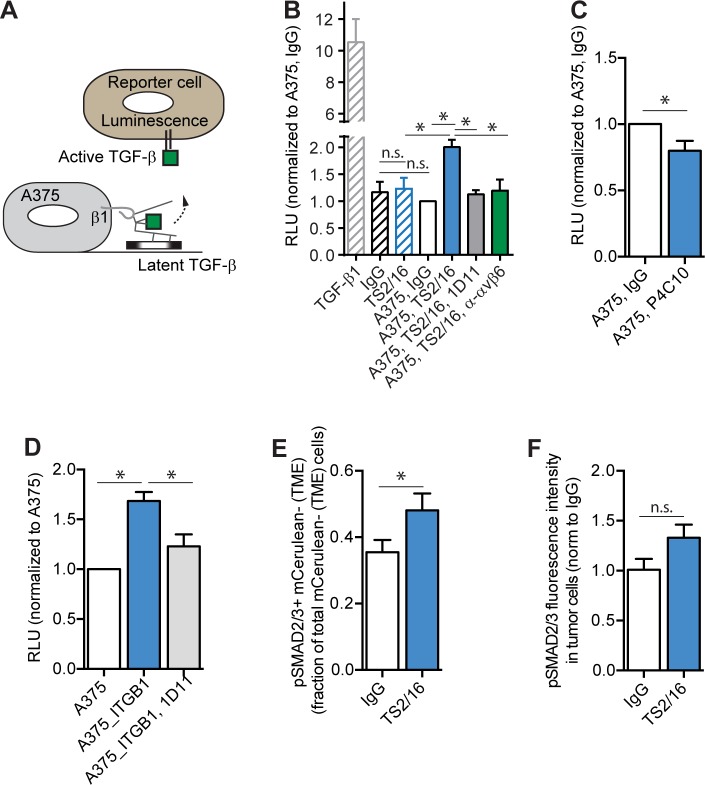
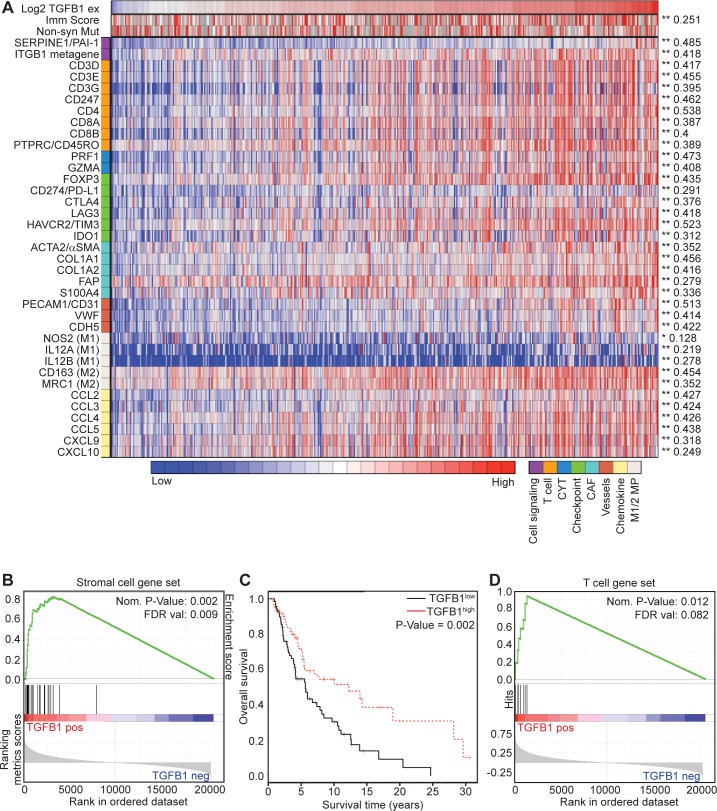
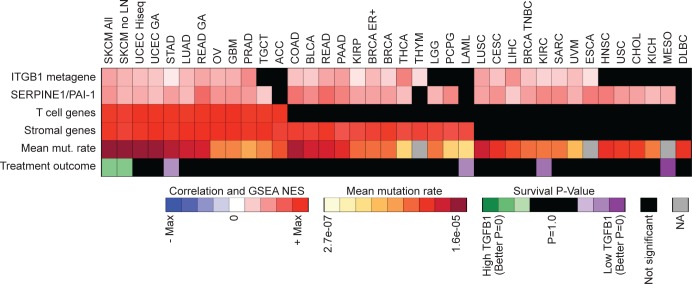
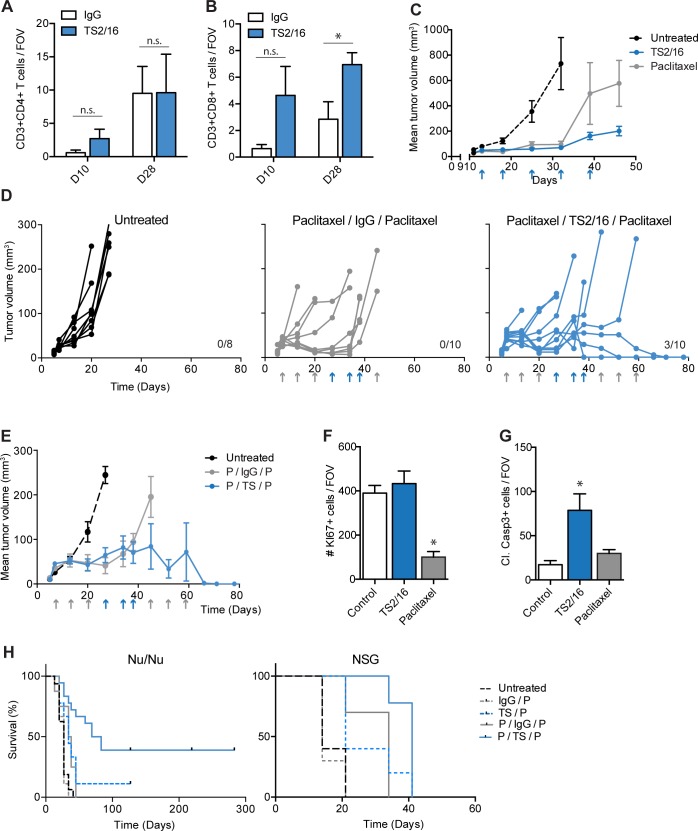
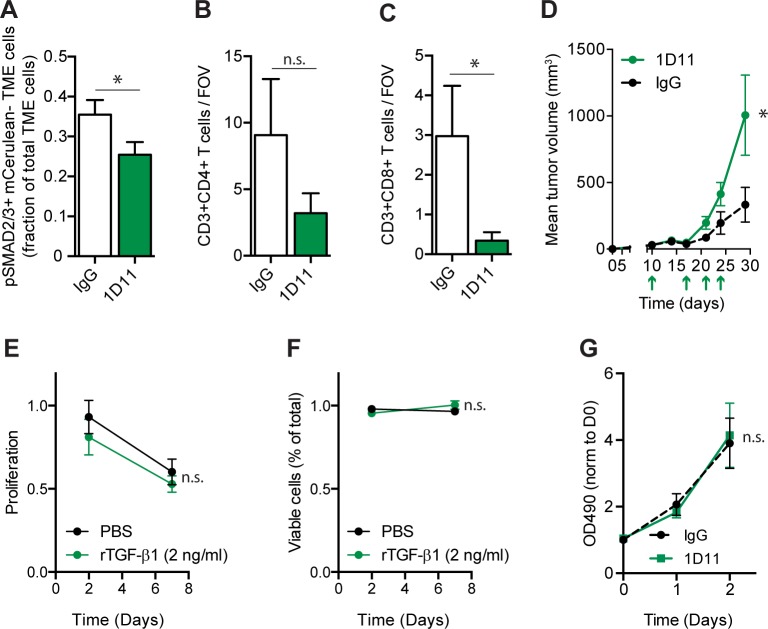
TGF-β is a cytokine thought to function as a tumor promoter in advanced malignancies. In this setting, TGF-β increases cancer cell proliferation, survival, and migration, and orchestrates complex, pro-tumorigenic changes in the tumor microenvironment. Here, we find that in melanoma, integrin β1-mediated TGF-β activation may also produce tumor suppression via an altered host response. In the A375 human melanoma cell nu/nu xenograft model, we demonstrate that cell surface integrin β1-activation increases TGF-β activity, resulting in stromal activation, neo-angiogenesis and, unexpectedly for this nude mouse model, increase in the number of intra-tumoral CD8+ T lymphocytes within the tumor microenvironment. This is associated with attenuation of tumor growth and long-term survival benefit. Correspondingly, in human melanomas, TGF-β1 correlates with integrin β1/TGF-β1 activation and the expression of markers for vasculature and stromal activation. Surprisingly, this integrin β1/TGF-β1 transcriptional footprint also correlates with the expression of markers for tumor-infiltrating lymphocytes, multiple immune checkpoints and regulatory pathways, and, importantly, better long-term survival of patients. These correlations are unique to melanoma, in that we do not observe similar associations between β1 integrin/TGF-β1 activation and better long-term survival in other human tumor types. These results suggest that activation of TGF-β1 in melanoma may be associated with the generation of an anti-tumor host response that warrants further study.
Conflict of interest statement
Figures
References
-
- Soengas MS, Lowe SW (2003) Apoptosis and melanoma chemoresistance. Oncogene 22: 3138–3151. doi: 10.1038/sj.onc.1206454 - DOI - PubMed
-
- Sosman JA, Kim KB, Schuchter L, Gonzalez R, Pavlick AC, et al. (2012) Survival in BRAF V600-mutant advanced melanoma treated with vemurafenib. N Engl J Med 366: 707–714. doi: 10.1056/NEJMoa1112302 - DOI - PMC - PubMed
-
- Puzanov I, Amaravadi RK, McArthur GA, Flaherty KT, Chapman PB, et al. (2015) Long-term outcome in BRAF(V600E) melanoma patients treated with vemurafenib: Patterns of disease progression and clinical management of limited progression. Eur J Cancer 51: 1435–1443. doi: 10.1016/j.ejca.2015.04.010 - DOI - PMC - PubMed
-
- Shi H, Hugo W, Kong X, Hong A, Koya RC, et al. (2014) Acquired resistance and clonal evolution in melanoma during BRAF inhibitor therapy. Cancer Discov 4: 80–93. doi: 10.1158/2159-8290.CD-13-0642 - DOI - PMC - PubMed
-
- Van Allen EM, Wagle N, Sucker A, Treacy DJ, Johannessen CM, et al. (2014) The genetic landscape of clinical resistance to RAF inhibition in metastatic melanoma. Cancer Discov 4: 94–109. doi: 10.1158/2159-8290.CD-13-0617 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
