

Vasopressor use following traumatic injury - A single center retrospective study
- PMID: 28448605
- PMCID: PMC5407798
- DOI: 10.1371/journal.pone.0176587
Vasopressor use following traumatic injury - A single center retrospective study
Abstract
Objectives: Vasopressors are not recommended by current trauma guidelines, but recent reports indicate that they are commonly used. We aimed to describe the early hemodynamic management of trauma patients outside densely populated urban centers.
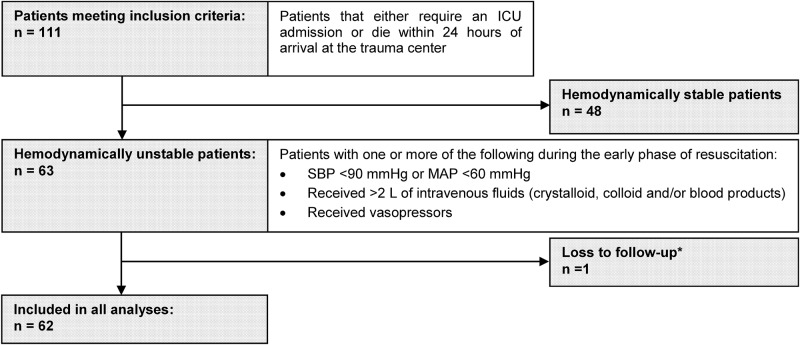
Methods: We conducted a single-center retrospective cohort study in a Canadian regional trauma center. All adult patients treated for traumatic injury in 2013 who died within 24 hours of admission or were transferred to the intensive care unit were included. A systolic blood pressure <90 mmHg, a mean arterial pressure <60 mmHg, the use of vasopressors or ≥2 L of intravenous fluids defined hemodynamic instability. Main outcome measures were use of intravenous fluids and vasopressors prior to surgical or endovascular management.
Results: Of 111 eligible patients, 63 met our criteria for hemodynamic instability. Of these, 60 (95%) had sustained blunt injury and 22 (35%) had concomitant severe traumatic brain injury. The subgroup of patients referred from a primary or secondary hospital (20 of 63, 32%) had significantly longer transport times (243 vs. 61 min, p<0.01). Vasopressors, used in 26 patients (41%), were independently associated with severe traumatic brain injury (odds ratio 10.2, 95% CI 2.7-38.5).
Conclusions: In this cohort, most trauma patients had suffered multiple blunt injuries. Patients were likely to receive vasopressors during the early phase of trauma care, particularly if they exhibited signs of neurologic injury. While these results may be context-specific, determining the risk-benefit trade-offs of fluid resuscitation, vasopressors and permissive hypotension in specific patients subgroups constitutes a priority for trauma research going forwards.
Conflict of interest statement
Figures
References
-
- Teixeira PG, Inaba K, Hadjizacharia P, Brown C, Salim A, Rhee P, et al. Preventable or potentially preventable mortality at a mature trauma center. J Trauma Acute Care Surg. 2007;63(6):1338–47. - PubMed
-
- Tien HC, Spencer F, Tremblay LN, Rizoli SB, Brenneman FD. Preventable deaths from hemorrhage at a level I Canadian trauma center. J Trauma Acute Care Surg. 2007;62(1):142–6. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
