

A meta-analysis comparing the risk of metastases in patients with rectal cancer and MRI-detected extramural vascular invasion (mrEMVI) vs mrEMVI-negative cases
- PMID: 28449006
- PMCID: PMC5518867
- DOI: 10.1038/bjc.2017.99
A meta-analysis comparing the risk of metastases in patients with rectal cancer and MRI-detected extramural vascular invasion (mrEMVI) vs mrEMVI-negative cases
Abstract
Background: Pathological extramural vascular invasion (EMVI) is an independent prognostic factor in rectal cancer, but can also be identified on MRI-detected extramural vascular invasion (mrEMVI). We perform a meta-analysis to determine the risk of metastatic disease at presentation and after surgery in mrEMVI-positive patients compared with negative tumours.
Methods: Electronic databases were searched from January 1980 to March 2016. Conventional meta-analytical techniques were used to provide a summative outcome. Quality assessment of the studies was performed.
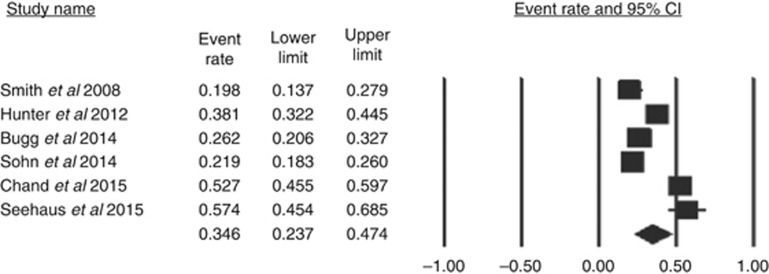
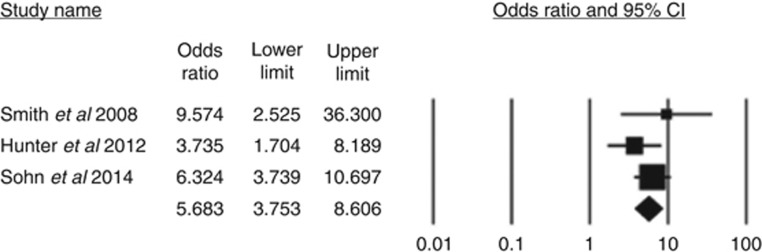
Results: Six articles reported on mrEMVI in 1262 patients. There were 403 patients in the mrEMVI-positive group and 859 patients in the mrEMVI-negative group. The combined prevalence of mrEMVI-positive tumours was 0.346(range=0.198-0.574). Patients with mrEMVI-positive tumours presented more frequently with metastases compared to mrEMVI-negative tumours (fixed effects model: odds ratio (OR)=5.68, 95% confidence interval (CI) (3.75, 8.61), z=8.21, df=2, P<0.001). Patients who were mrEMVI-positive developed metastases more frequently during follow-up (random effects model: OR=3.91, 95% CI (2.61, 5.86), z=6.63, df=5, P<0.001).
Conclusions: MRI-detected extramural vascular invasion is prevalent in one-third of patients with rectal cancer. MRI-detected extramural vascular invasion is a poor prognostic factor as evidenced by the five-fold increased rate of synchronous metastases, and almost four-fold ongoing risk of developing metastases in follow-up after surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Additional value of MRI-detected EMVI scoring system in rectal cancer: applicability in predicting synchronous metastasis.Tumori. 2020 Aug;106(4):286-294. doi: 10.1177/0300891620901745. Epub 2020 Mar 2. Tumori. 2020. PMID: 32116150
-
The prognostic importance of MRI detected extramural vascular invasion (mrEMVI) in locally advanced rectal cancer.Int J Colorectal Dis. 2020 Oct;35(10):1849-1854. doi: 10.1007/s00384-020-03632-9. Epub 2020 Jun 2. Int J Colorectal Dis. 2020. PMID: 32488420
-
Risk of nodal disease in patients with MRI-detected extramural vascular invasion in rectal cancer: a systematic review and meta-analysis.Tumori. 2021 Dec;107(6):564-570. doi: 10.1177/0300891620975867. Epub 2020 Nov 26. Tumori. 2021. PMID: 33243105
-
The prognostic value of MRI-detected extramural vascular invasion (mrEMVI) for rectal cancer patients treated with neoadjuvant therapy: a meta-analysis.Eur Radiol. 2021 Dec;31(12):8827-8837. doi: 10.1007/s00330-021-07981-z. Epub 2021 May 15. Eur Radiol. 2021. PMID: 33993333 Review.
-
Association between high-resolution MRI-detected extramural vascular invasion and tumour microcirculation estimated by dynamic contrast-enhanced MRI in rectal cancer: preliminary results.BMC Cancer. 2019 May 27;19(1):498. doi: 10.1186/s12885-019-5732-z. BMC Cancer. 2019. PMID: 31133005 Free PMC article.
Cited by
-
MRI Assessment of Extramural Venous Invasion Before and After Total Neoadjuvant Therapy for Locally Advanced Rectal Cancer and Its Association with Disease-Free and Overall Survival.Ann Surg Oncol. 2023 Jul;30(7):3957-3965. doi: 10.1245/s10434-023-13225-9. Epub 2023 Mar 24. Ann Surg Oncol. 2023. PMID: 36964328 Free PMC article.
-
Metastasis risk stratification and response prediction through dynamic viable circulating tumor cell counts for rectal cancer in a neoadjuvant setting.Cancer Med. 2023 May;12(10):11438-11450. doi: 10.1002/cam4.5860. Epub 2023 Apr 4. Cancer Med. 2023. PMID: 37014817 Free PMC article.
-
Personalized Treatment Modalities for Rectal Cancer: Advances in Neoadjuvant Treatment.J Clin Med. 2025 Jun 20;14(13):4411. doi: 10.3390/jcm14134411. J Clin Med. 2025. PMID: 40648785 Free PMC article. Review.
-
Addition of Platinum Derivatives to Fluoropyrimidine-Based Neoadjuvant Chemoradiotherapy for Stage II/III Rectal Cancer: Systematic Review and Meta-Analysis.J Natl Cancer Inst. 2019 Sep 1;111(9):887-902. doi: 10.1093/jnci/djz081. J Natl Cancer Inst. 2019. PMID: 31077329 Free PMC article.
-
A Comprehensive Evaluation of Associations Between Routinely Collected Staging Information and The Response to (Chemo)Radiotherapy in Rectal Cancer.Cancers (Basel). 2020 Dec 22;13(1):16. doi: 10.3390/cancers13010016. Cancers (Basel). 2020. PMID: 33375133 Free PMC article.
References
-
- Battersby NJ, How P, Moran B, Stelzner S, West NP, Branagan G, Strassburg J, Quirke P, Tekkis P, Pedersen BG, Gudgeon M, Heald B, Brown G Group, MIS (2016) Prospective validation of a low rectal cancer magnetic resonance imaging staging system and development of a local recurrence risk stratification model: The MERCURY II Study. Ann Surg 263: 751–760. - PubMed
-
- Betge J, Pollheimer MJ, Lindtner RA, Kornprat P, Schlemmer A, Rehak P, Vieth M, Hoefler G, Langner C (2012) Intramural and extramural vascular invasion in colorectal cancer: prognostic significance and quality of pathology reporting. Cancer 118: 628–638. - PubMed
-
- Bhangu A, Fitzgerald JE, Slesser A, Northover JM, Faiz O, Tekkis P (2013) Prognostic significance of extramural vascular invasion in T4 rectal cancer. Colorectal Dis 15: e665–e671. - PubMed
-
- Borenstein M, HL, Higgins J, Rothstein H (ed.) (2005) ComprehensiveMeta-analysis Version 2. Englewood, NJ, USA.
-
- Brown CE, Warren S (1938) Visceral metastasis from rectal carcinoma. Surg Gynecol Obstet 66: 611–621.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
