

Marijuana Use Impacts Midlife Cardiovascular Events in HIV-Infected Men
- PMID: 28449059
- PMCID: PMC5850013
- DOI: 10.1093/cid/cix391
Marijuana Use Impacts Midlife Cardiovascular Events in HIV-Infected Men
Abstract
Background: Marijuana use is prevalent among persons infected with human immunodeficiency virus (HIV), but its long-term effects on HIV disease progression and comorbidities are unknown.
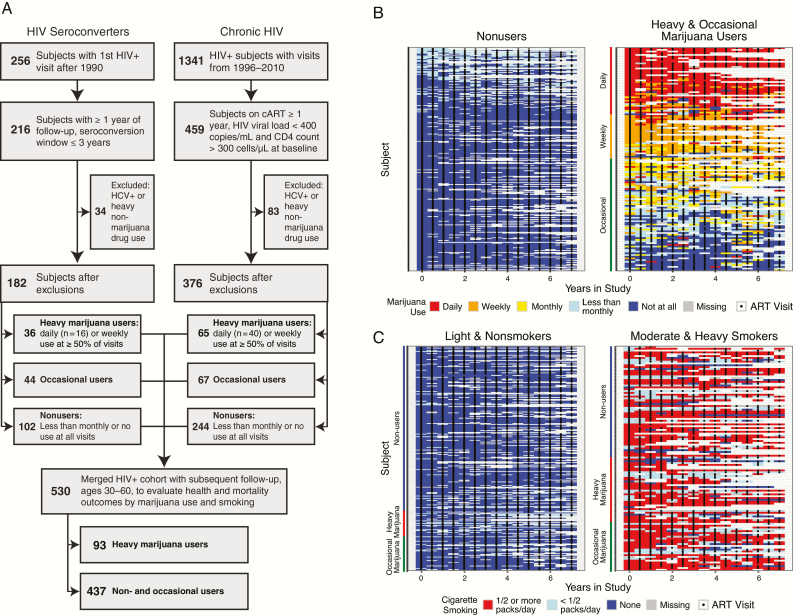
Methods: In this prospective study of 558 HIV-infected men enrolled in the Multicenter AIDS Cohort Study between 1990 and 2010, there were 182 HIV seroconverters and 376 with viral suppression on combination antiretroviral therapy (ART). Associations between heavy marijuana use and HIV disease markers or white blood cell (WBC) count were examined using mixed-effects and linear regression models. Effects of marijuana use on cardiovascular (CV) events and other endpoints were estimated using Kaplan-Meier and logistic regression analyses.
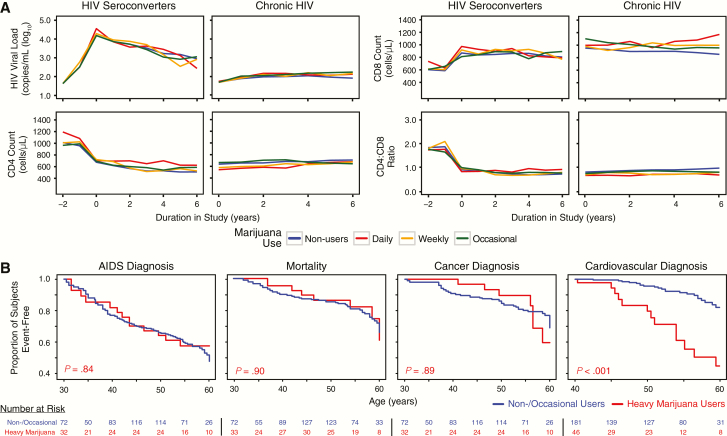
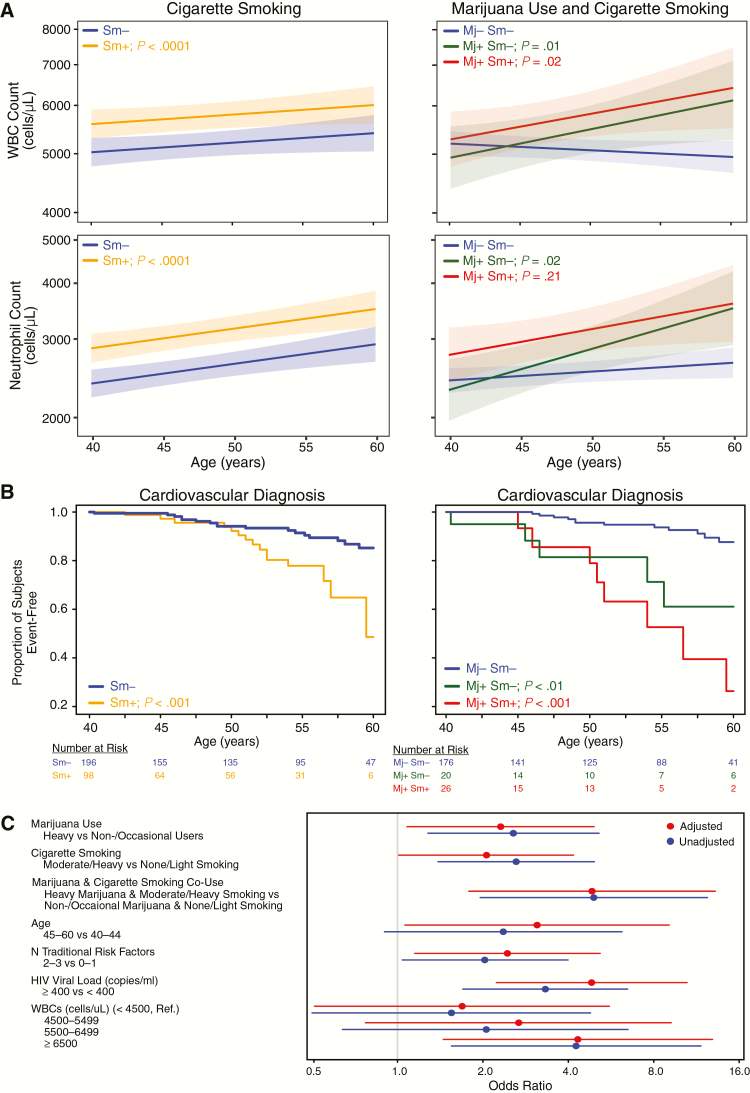
Results: The median baseline age of participants was 41, 66% were white, 79% had education >12 years, and 20% reported heavy marijuana use at ≥50% of biannual visits during follow-up. Long-term heavy marijuana use showed no significant associations with viral load, CD4 counts, AIDS, cancer, or mortality in both cohorts but was independently associated with increased CV events between ages 40-60 after adjusting for age, tobacco smoking, viral load, and traditional risk factors (odds ratio [OR], 2.5; 95% confidence interval [CI] 1.3, 5.1). Marijuana and tobacco use were each independently associated with higher WBC counts in adjusted models (P < .01); the highest quartile of WBC counts (≥6500 cells/µL) was associated with increased CV events (OR 4.3; 95% CI, 1.5, 12.9).
Conclusions: Heavy marijuana use is a risk factor for CV disease in HIV-infected men ages 40-60, independent of tobacco smoking and traditional risk factors.
Keywords: AIDS; HIV; cardiovascular disease; marijuana.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- National Academies of Sciences, Engineering, and Medicine. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington (DC): The National Academies Press, 2017. - PubMed
-
- Abrams DI, Hilton JF, Leiser RJ et al. Short-term effects of cannabinoids in patients with HIV-1 infection: a randomized, placebo-controlled clinical trial. Ann Intern Med 2003; 139:258–66. - PubMed
MeSH terms
Grants and funding
- U01 AI035041/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- R01 DA030985/DA/NIDA NIH HHS/United States
- DP1 DA028994/DA/NIDA NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- R01 AI116744/AI/NIAID NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
