

Efficacy and safety of lixisenatide in patients with type 2 diabetes and renal impairment
- PMID: 28449324
- PMCID: PMC5655920
- DOI: 10.1111/dom.12986
Efficacy and safety of lixisenatide in patients with type 2 diabetes and renal impairment
Abstract
Aims: This post hoc assessment evaluated the efficacy and safety of once-daily, prandial glucagon-like peptide-1 receptor agonist lixisenatide in patients with type 2 diabetes (T2D) and normal renal function (estimated glomerular filtration rate ≥90 mL/min), or mild (60-89 mL/min) or moderate (30-59 mL/min) renal impairment.
Methods: Patients from 9 lixisenatide trials in the GetGoal clinical trial programme were categorized by baseline creatinine clearance: normal renal function (lixisenatide n = 2094, placebo n = 1150); renal impairment (mild: lixisenatide n = 637, placebo n = 414; moderate: lixisenatide n = 122, placebo n = 68). Meta-analyses of placebo-adjusted mean differences between baseline renal categories were performed for efficacy and safety outcomes.
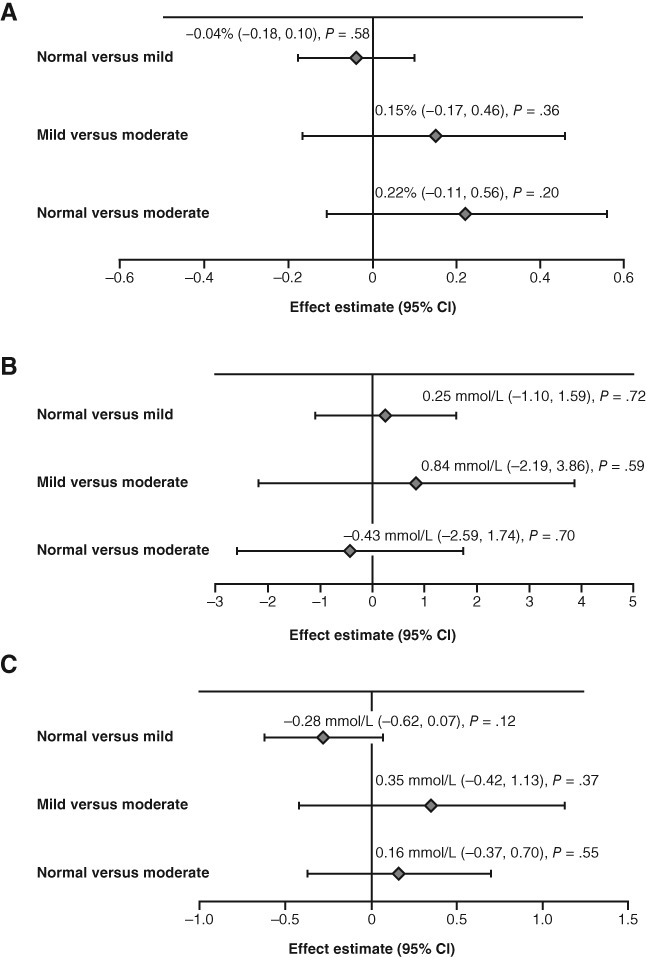
Results: HbA1c, 2-hour postprandial plasma glucose and fasting plasma glucose were comparably reduced in lixisenatide-treated patients with normal renal function, and mild and moderate renal impairment. The most common adverse events (AEs) in all renal function categories were gastrointestinal (GI), predominantly nausea and vomiting. A 14% higher incidence of GI AEs and a 10% higher incidence of nausea and vomiting were seen with mild impairment vs normal function (P = .003 for both), but no significant differences were observed between the mild and moderate impairment categories (P = .99 and P = .57, respectively), or between the moderate impairment and normal categories (P = .16 and P = .65, respectively). Additionally, the incidence of hypoglycaemia was similar in all categories.
Conclusions: This study demonstrates that baseline renal status does not affect efficacy outcomes in lixisenatide- vs placebo-treated patients, and that no lixisenatide dose adjustment is required for patients with T2D with mild or moderate renal impairment.
Keywords: GLP-1; incretin therapy; meta-analysis; type 2 diabetes.
© 2017 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
M. H. has served on an advisory panel and as an author for Bristol‐Myers Squibb, GlaxoSmithKline, Sanofi and Takeda; and has served on a speakers’ bureau and as an author for Bayer Health Care, Eli Lilly, GlaxoSmithKline, Roche, Sanofi and Takeda. J. M. A. has served on an advisory panel and as an author for AstraZeneca, Bristol‐Myers Squibb, Novo Nordisk and Sanofi; and as a speaker for Sanofi. L. A. L. has received research funding from, has provided CME on behalf of, and/or has served as an adviser to AstraZeneca, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, Janssen, Merck, Novo Nordisk, Pfizer, Sanofi, Servier and Takeda. G. M. has received research support from and served as an author for MSD; has served on a speakers’ bureau and as an author for Boehringer Ingelheim, Eli Lilly, MSD, Novartis, Novo Nordisk and Sanofi; and has served on an advisory panel for Boehringer Ingelheim, Eli Lilly and Sanofi. E. N. is an employee of Artech Information Systems, under contract with Sanofi as a clinical data associate. M. S. has served on an advisory panel and as an author for Novo Nordisk; has received research support from and served as an author for Novartis; and has served on speakers’ bureau and as an author for AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Eli Lilly, MSD, Novartis, Novo Nordisk and Servier. W. S. is an employee of Sanofi. R. G.‐H. has served on an advisory panel and as an author for Boehringer Ingelheim, Eli Lilly, Janssen, Novo Nordisk and Sanofi.
Figures
Similar articles
-
Postprandial renal haemodynamic effect of lixisenatide vs once-daily insulin-glulisine in patients with type 2 diabetes on insulin-glargine: An 8-week, randomised, open-label trial.Diabetes Obes Metab. 2017 Dec;19(12):1669-1680. doi: 10.1111/dom.12985. Epub 2017 Jul 25. Diabetes Obes Metab. 2017. PMID: 28449402 Clinical Trial.
-
Efficacy and safety of lixisenatide as add-on therapy to basal insulin in older adults with type 2 diabetes in the GetGoal-O Study.J Diabetes. 2019 Dec;11(12):971-981. doi: 10.1111/1753-0407.12952. Epub 2019 Jun 26. J Diabetes. 2019. PMID: 31094074 Free PMC article. Clinical Trial.
-
Beneficial effect of lixisenatide after 76 weeks of treatment in patients with type 2 diabetes mellitus: A meta-analysis from the GetGoal programme.Diabetes Obes Metab. 2017 Feb;19(2):248-256. doi: 10.1111/dom.12810. Epub 2016 Dec 8. Diabetes Obes Metab. 2017. PMID: 27762096
-
Lixisenatide, a novel GLP-1 receptor agonist: efficacy, safety and clinical implications for type 2 diabetes mellitus.Diabetes Obes Metab. 2014 Jul;16(7):588-601. doi: 10.1111/dom.12253. Epub 2014 Jan 20. Diabetes Obes Metab. 2014. PMID: 24373190 Review.
-
Lixisenatide: A New Daily GLP-1 Agonist for Type 2 Diabetes Management.Ann Pharmacother. 2017 May;51(5):401-409. doi: 10.1177/1060028017689878. Epub 2017 Jan 29. Ann Pharmacother. 2017. PMID: 28133970 Review.
Cited by
-
Review of glucagon-like peptide-1 receptor agonists for the treatment of type 2 diabetes mellitus in patients with chronic kidney disease and their renal effects.J Diabetes. 2019 Dec;11(12):938-948. doi: 10.1111/1753-0407.12969. Epub 2019 Aug 14. J Diabetes. 2019. PMID: 31318152 Free PMC article. Review.
-
Glucagon-like peptide 1 (GLP-1) receptor agonists for people with chronic kidney disease and diabetes.Cochrane Database Syst Rev. 2025 Feb 18;2(2):CD015849. doi: 10.1002/14651858.CD015849.pub2. Cochrane Database Syst Rev. 2025. PMID: 39963952
-
Advances in the management of diabetic kidney disease: beyond sodium-glucose co-transporter 2 inhibitors.Kidney Res Clin Pract. 2022 Nov;41(6):682-698. doi: 10.23876/j.krcp.21.285. Epub 2022 Jul 19. Kidney Res Clin Pract. 2022. PMID: 35977903 Free PMC article.
-
Pharmacokinetics, Safety and Tolerability of Oral Semaglutide in Subjects with Renal Impairment.Clin Pharmacokinet. 2018 Dec;57(12):1571-1580. doi: 10.1007/s40262-018-0649-2. Clin Pharmacokinet. 2018. PMID: 29623579 Free PMC article. Clinical Trial.
-
Consensus Recommendations on GLP-1 RA Use in the Management of Type 2 Diabetes Mellitus: South Asian Task Force.Diabetes Ther. 2019 Oct;10(5):1645-1717. doi: 10.1007/s13300-019-0669-4. Epub 2019 Jul 29. Diabetes Ther. 2019. PMID: 31359367 Free PMC article. Review.
References
-
- Gilbert RE. Endothelial loss and repair in the vascular complications of diabetes: pathogenetic mechanisms and therapeutic implications. Circ J. 2013;77:849‐856. - PubMed
-
- Molitch ME. Current state of type 2 diabetes management. Am J Manag Care. 2013;19:S136‐S142. - PubMed
-
- MacCallum L. Optimal medication dosing in patients with diabetes mellitus and chronic kidney disease. Can J Diabetes. 2014;38:334‐343. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
