

Pulmonary inflammatory myofibroblastic tumor versus IgG4-related inflammatory pseudotumor: differential diagnosis based on a case series
- PMID: 28449468
- PMCID: PMC5394068
- DOI: 10.21037/jtd.2017.02.89
Pulmonary inflammatory myofibroblastic tumor versus IgG4-related inflammatory pseudotumor: differential diagnosis based on a case series
Abstract
Background: Pulmonary inflammatory myofibroblastic tumor (IMT) has been considered as a synonym for inflammatory pseudotumor (IPT) for a long time. Recent studies have indicated that IMT and IgG4-related IPT are distinct diseases. However, no consensus criteria have been recommended. Here we propose a set of criteria for the differential diagnosis.
Methods: Twenty-six archived IMT and IgG4-related IPT samples were examined for histological characteristics and the expression of IgG, IgG4, SMA and ALK-1. Based on our proposed criteria, we reclassified the cases into either IMT or IgG4-related IPT group and compared the clinicopathological features, laboratory findings, overall survivals (OS) and disease-free survivals between groups to validate the effectiveness and dependability of the diagnostic criteria.
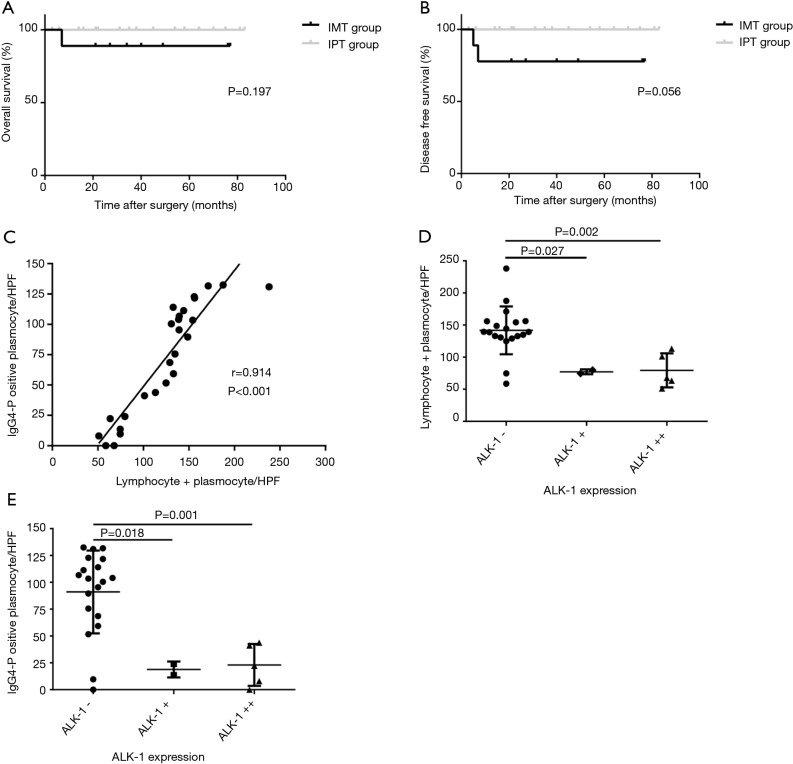
Results: The average age of IgG4-related IPT group was higher than IMTs (48.82 vs. 39.22 years, P=0.031). In IMT group, tumors were characterized by bigger tumor sizes (3.47 vs. 2.22 cm, P=0.007), diffuse and total destroyed alveoli (88.89% vs. 17.65%, P=0.002), fewer lymphoid follicles (1.6/HPF vs. 3.0/HPF, P=0.045) and lower expression of IgG (74.7/HPF vs. 149.1/HPF; P<0.001). As an exclusion criterion of IgG4-related IPT, ALK-positivity was correlated with the higher cytological atypia (mean 3.7/HPF, P<0.001) and lesser lymphoid follicles (mean 1.2/HPF, P=0.021). And it's the first study to show the liner positive correlation between the lymphocytes + plasma cells count and IgG4-positive plasma cells count in these lesions (r=0.914, P<0.001). The negative correlation between the IgG4-positive plasma cells count and the expression of ALK-1 are reported for the first time as well (rs=-0.632, P=0.001). However, despite two patients with recurrence or metastasis were divided into IMT group, only borderline values were detected in the survival analysis (OS 88.89% vs. 100%, P=0.197, DFS 77.78% vs. 100.00%; P=0.056).
Conclusions: The significant differences of clinicopathological characteristics between the IMTs and IgG4-related IPTs indicated that a combination of lymphocytes + plasma cells count, cytological atypia, IgG4 and ALK-1 staining will be helpful in differential diagnosis.
Keywords: Inflammatory myofibroblastic tumor (IMT); differential diagnosis; inflammatory pseudotumor (IPT).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Travis WD, Brambilla E, Muller-Hermelink HK, et al. Pathology and Genetics of Tumours of the Lung, Pleura,Thymus and Heart. IARC Press, International Agency for Research on Cancer. 2004.
-
- Griffin CA, Hawkins AL, Dvorak C, et al. Recurrent involvement of 2p23 in inflammatory myofibroblastic tumors. Cancer Res 1999;59:2776-80. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials