

Clinical presentation and characteristics of 25 adult cases of pulmonary sequestration
- PMID: 28449484
- PMCID: PMC5393996
- DOI: 10.21037/jtd.2017.03.107
Clinical presentation and characteristics of 25 adult cases of pulmonary sequestration
Abstract
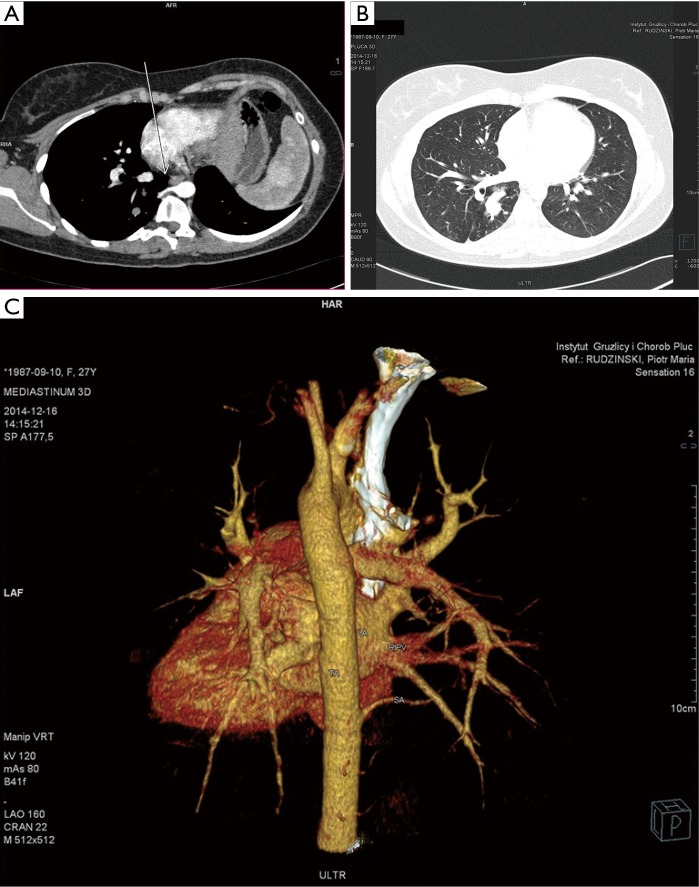
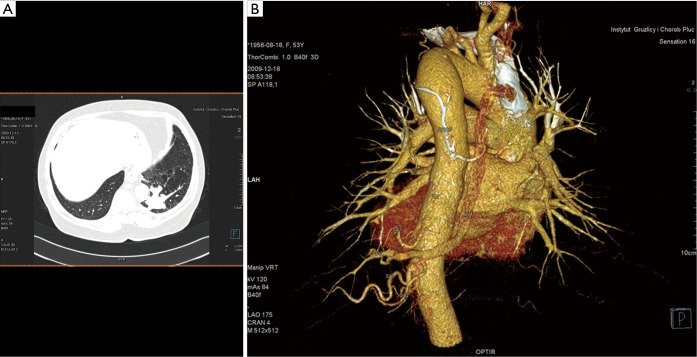
Background: Pulmonary sequestration (PS) is a rare congenital abnormality of lung tissue. Only few series of adult cases are reported. The aim was to describe clinical characteristics in adult cases of PS and to compare outcomes in different clinical situations.
Methods: Using MSD engine we searched for cases of PS that have been diagnosed between Jan 1st, 2005 and Dec 31st, 2015. Clinical data was retrospectively gathered. Statistica v.12 (StatSoft, Inc.) was used for statistical analyses.
Results: We found 25 cases (18 females, 7 males), which underwent surgery and were histologically proven. There were 22 cases of intralobar PS. 7 cases were asymptomatic, 12 had infectious history (including 3 cases of lung abscess and pleural empyema), 4 presented with hemoptysis, 2 with chest pain. The average age to undergo surgery was 38.24, in the asymptomatic group 34, in symptomatic 39.89. In the latter the symptoms preceded the surgery for 2.45-year. Great majority of sequestrations was located in lower lobes (96%), 52% on the left. Symptomatic cases were at higher than expected risk of surgical complications, comparing to asymptomatic (chi2, P=0.04). In most cases there were surgical and histological signs of infection, only in 9 cases etiological factor was determined: in 5 cases it was A. fumigatus. A 0.53-day longer post-surgical hospital stay was observed in the symptomatic group, no statistical significance was found (U-test, P=0.45).
Conclusions: Surgical treatment of symptomatic cases of PS is characterized by slightly longer post-surgical hospital stay and higher risk of surgical complications. Fungal infections are the most likely to occur in PS.
Keywords: Congenital malformation; aspergillosis; recurrent infection.
Conflict of interest statement
Conflicts of Interest: This work was presented on 2016 ERS International Congress London, on Sep 4, 2016.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials