

Malignant pheochromocytoma in the anterior mediastinum with sternal invasion: a case report
- PMID: 28449504
- PMCID: PMC5394084
- DOI: 10.21037/jtd.2017.02.71
Malignant pheochromocytoma in the anterior mediastinum with sternal invasion: a case report
Abstract
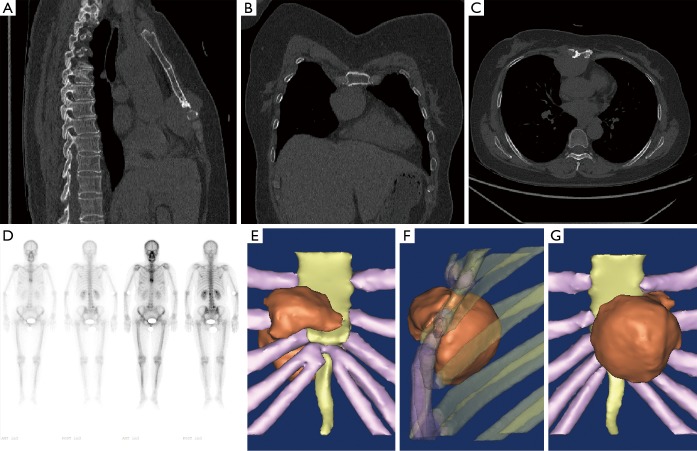
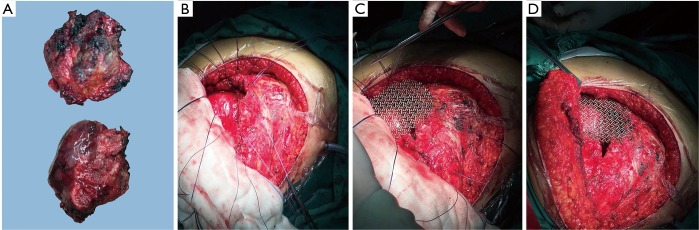
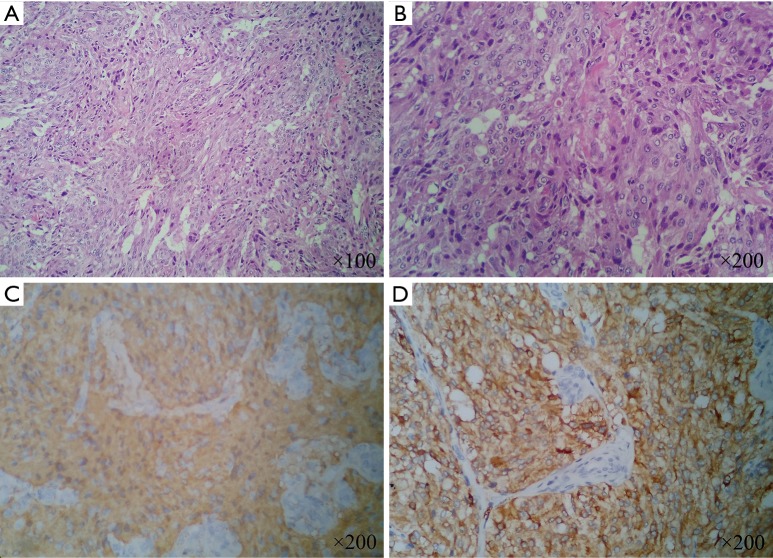
Pheochromocytomas are catecholamine-producing neuroendocrine tumors that usually occur in the adrenal medulla or sympathetic paraganglia. Anterior mediastinum involvement with pheochromocytoma is rare and may not present with typical symptoms. Its clinical manifestation may be unclear and a high index of suspicion is required for accurate diagnosis. We report a rare case of pheochromocytoma of the anterior mediastinum in a 51-year-old female. A painful hard mass on the sternum was the only clinical manifestation. Imageological examination indicated that there might be a malignant mass on the anterior mediastinum and thoracic wall. The patient accepted surgical curettage and thoracic wall reconstruction. Based on pathological results and WHO definition, the final diagnosis was malignant pheochromocytoma. After six months follow-up, the patient had no recurrence or any symptom. Malignant pheochromocytoma in the anterior mediastinum invading the sternum is rare. A local painful mass may be the only clinical manifestation without special laboratory results. Surgery remains as the first choice for these patients. For this rare case, 3D reconstruction by special software may be a good method to realize individualized treatment. The final decision of the diagnosis should be based on pathological results, past medical history and WHO definition. Long-term follow-up is necessary, while other suspicious lesions should also be given sufficient attention.
Keywords: Pheochromocytoma; sternum; surgery; thoracic wall; three-dimensional (3D) reconstruction.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous