

Surgical resection of right ventricular rhabdomyoma under the guidance of transesophageal echocardiography on a beating heart
- PMID: 28449506
- PMCID: PMC5393986
- DOI: 10.21037/jtd.2017.02.63
Surgical resection of right ventricular rhabdomyoma under the guidance of transesophageal echocardiography on a beating heart
Abstract
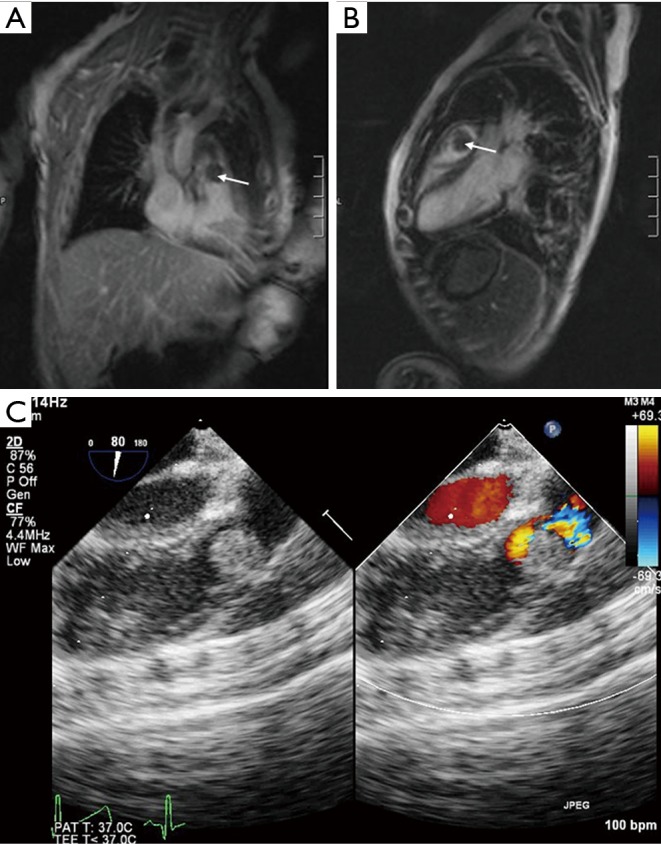
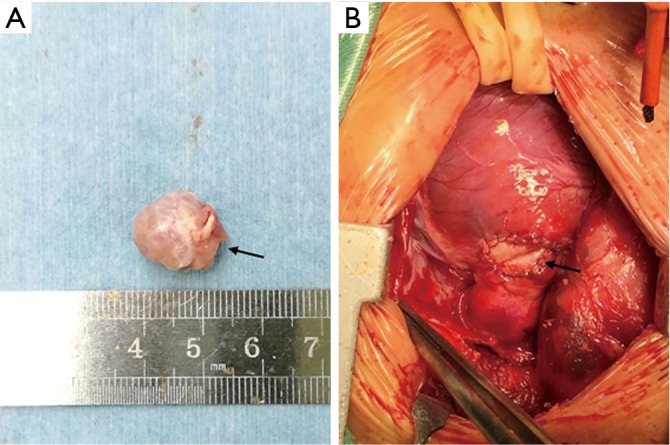
Cardiac rhabdomyoma, a type of benign myocardial tumor, is regarded as the most common fetal cardiac tumor. Rhabdomyomas are usually found before birth or during the first year of life. It is widely accepted that rhabdomyomas are strongly associated with tuberous sclerosis, and tend to regress spontaneously without surgical excision. However, if the tumor has caused significant obstruction or refractory arrhythmias, the surgery should be advocated. Most of the surgeries for pediatric cardiac tumors are performed under cardiopulmonary bypass (CPB) with cardioplegia. Here, we present a case of successful resection of a right ventricular rhabdomyoma obstructing the right ventricular outflow tract (RVOT) and involving pulmonary valve annulus in an infant, performed under the guidance of transesophageal echocardiography (TEE) on a beating heart.
Keywords: Cardiac rhabdomyoma; cardiopulmonary bypass (CPB); right ventricular outflow tract (RVOT); transesophageal echocardiography (TEE); transthoracic echocardiogram (TTE).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources