

Daily home fortification with iron as ferrous fumarate versus NaFeEDTA: a randomised, placebo-controlled, non-inferiority trial in Kenyan children
- PMID: 28449690
- PMCID: PMC5408380
- DOI: 10.1186/s12916-017-0839-z
Daily home fortification with iron as ferrous fumarate versus NaFeEDTA: a randomised, placebo-controlled, non-inferiority trial in Kenyan children
Abstract
Background: We aimed to show the non-inferiority of home fortification with a daily dose of 3 mg iron in the form of iron as ferric sodium ethylenediaminetetraacetate (NaFeEDTA) compared with 12.5 mg iron as encapsulated ferrous fumarate in Kenyan children aged 12-36 months. In addition, we updated a recent meta-analysis to assess the efficacy of home fortification with iron-containing powders, with a view to examining diversity in trial results.
Methods: We gave chemoprevention by dihydroartemisinin-piperaquine, albendazole and praziquantel to 338 afebrile children with haemoglobin concentration ≥70 g/L. We randomly allocated them to daily home fortification for 30 days with either placebo, 3 mg iron as NaFeEDTA or 12.5 mg iron as encapsulated ferrous fumarate. We assessed haemoglobin concentration (primary outcome), plasma iron markers, plasma inflammation markers and Plasmodium infection in samples collected at baseline and after 30 days of intervention. We conducted a meta-analysis of randomised controlled trials in pre-school children to assess the effect of home fortification with iron-containing powders on anaemia and haemoglobin concentration at end of intervention.
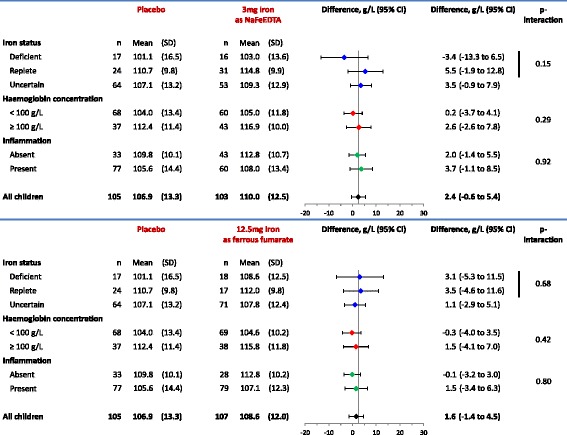
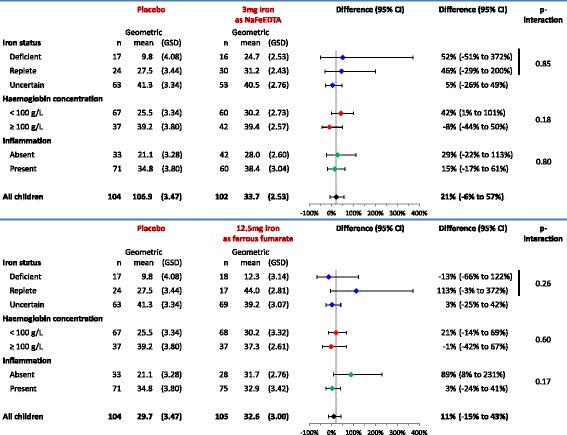
Results: A total of 315 children completed the 30-day intervention period. At baseline, 66.9% of children had inflammation (plasma C-reactive protein concentration >5 mg/L or plasma α 1-acid glycoprotein concentration >1.0 g/L); in those without inflammation, 42.5% were iron deficient. There was no evidence, either in per protocol analysis or intention-to-treat analysis, that home fortification with either of the iron interventions improved haemoglobin concentration, plasma ferritin concentration, plasma transferrin receptor concentration or erythrocyte zinc protoporphyrin-haem ratio. We also found no evidence of effect modification by iron status, anaemia status and inflammation status at baseline. In the meta-analysis, the effect on haemoglobin concentration was highly heterogeneous between trials (I 2: 84.1%; p value for test of heterogeneity: <0.0001).
Conclusions: In this population, home fortification with either 3 mg iron as NaFeEDTA or 12.5 mg iron as encapsulated ferrous fumarate was insufficiently efficacious to assess non-inferiority of 3 mg iron as NaFeEDTA compared to 12.5 mg iron as encapsulated ferrous fumarate. Our finding of heterogeneity between trial results should stimulate subgroup analysis or meta-regression to identify population-specific factors that determine efficacy.
Trial registration: The trial was registered with ClinicalTrials.gov ( NCT02073149 ) on 25 February 2014.
Keywords: Anaemia; Child; Ferric sodium EDTA; Home fortification; Iron; Meta-analysis; Non-inferiority; Pre-school.
Figures


Comment in
-
Micronutrient powders to combat anemia in young children: does it work?BMC Med. 2017 May 11;15(1):99. doi: 10.1186/s12916-017-0867-8. BMC Med. 2017. PMID: 28490333 Free PMC article.
-
Micronutrient powders to combat anaemia in young children: do they work?BMC Med. 2018 Jan 22;16(1):7. doi: 10.1186/s12916-017-0998-y. BMC Med. 2018. PMID: 29353552 Free PMC article.
References
-
- Use of multiple micronutrient powders for home fortification of foods consumed by infants and children 6–23 months of age. Geneva: World Health Organization; 2011. http://apps.who.int/iris/bitstream/10665/44651/1/9789241502047_eng.pdf. Accessed 8 Apr 2017. - PubMed
-
- Worldwide prevalence of anaemia 1993–2005: WHO Global Database on Anaemia. De Benoist, B, McLean E, Egli I, Cogswell M, editors. Geneva: World Health Organization; 2008. http://apps.who.int/iris/bitstream/10665/43894/1/9789241596657_eng.pdf. Accessed 30 Jan 2017.
-
- De-Regil LM, Suchdev PS, Vist GE, Walleser S, Peña-Rosas JP. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age. Cochrane Database Syst Rev. 2011;9:CD008959. - PubMed
-
- Nestel P, Alnwick D, for the International Nutritional Anaemia Consultative Group (INACG) Iron/multi-micronutrient supplements for young children: summary and conclusions of a consultation held at UNICEF, Copenhagen, August 19–20, 1996. Washington DC: ILSI Human Nutrition Institute; 1997.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
