

Young children with Down syndrome show normal development of circadian rhythms, but poor sleep efficiency: a cross-sectional study across the first 60 months of life
- PMID: 28449894
- PMCID: PMC5423393
- DOI: 10.1016/j.sleep.2016.12.026
Young children with Down syndrome show normal development of circadian rhythms, but poor sleep efficiency: a cross-sectional study across the first 60 months of life
Abstract
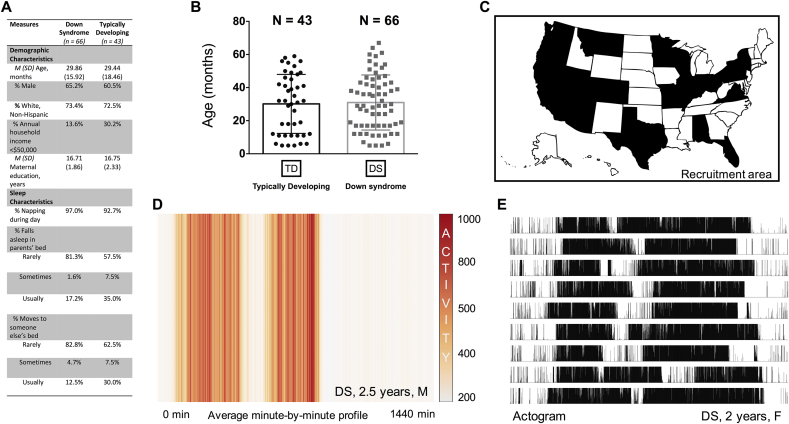
Objectives: To evaluate sleep consolidation and circadian activity rhythms in infants and toddlers with Down syndrome (DS) under light and socially entrained conditions within a familiar setting. Given previous human and animal data suggesting intact circadian regulation of melatonin across the day and night, it was hypothesized that behavioral indices of circadian rhythmicity would likewise be intact in the sample with DS.
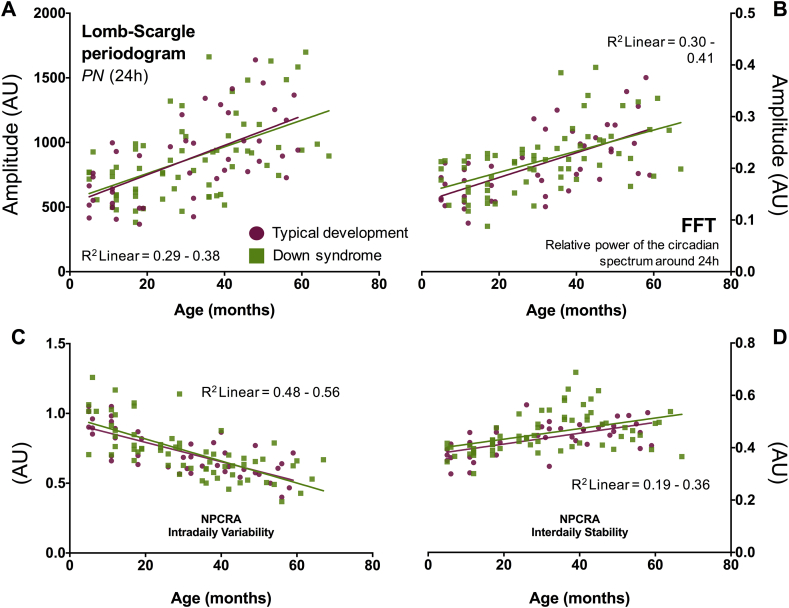
Methods: A cross-sectional study of 66 infants and young children with DS, aged 5-67 months, and 43 typically developing age-matched controls. Sleep and measures of circadian robustness or timing were quantified using continuous in-home actigraphy recordings performed over seven days. Circadian robustness was quantified via time series analysis of rest-activity patterns. Phase markers of circadian timing were calculated alongside these values. Sleep efficiency was also estimated based on the actigraphy recordings.
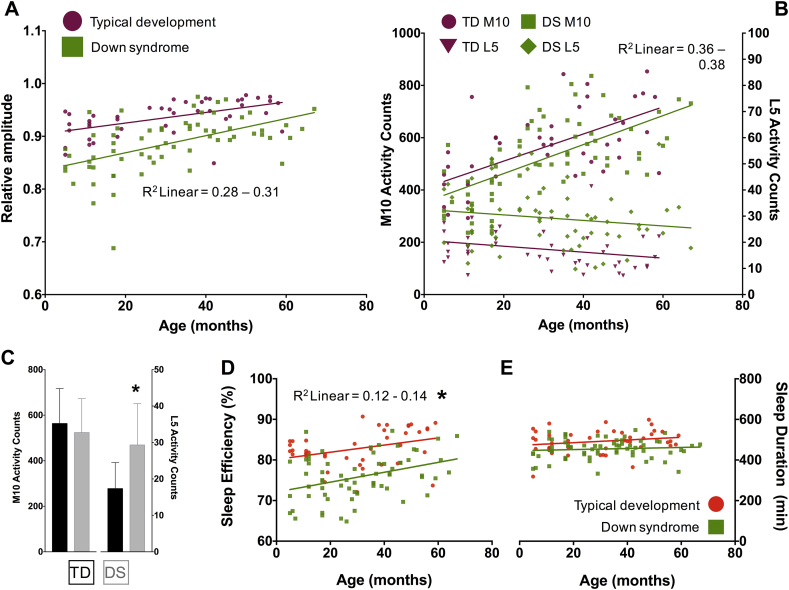
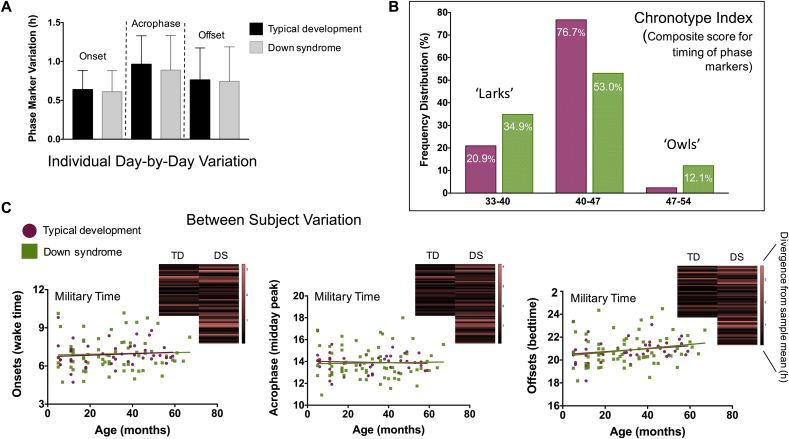
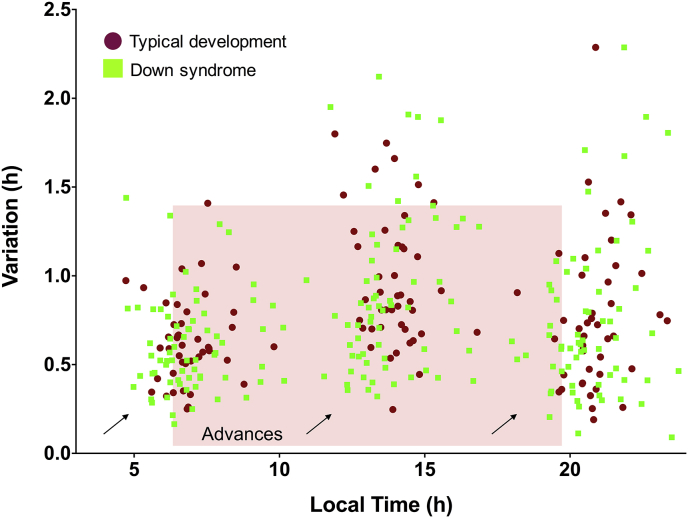
Results: This study provided further evidence that general sleep quality is poor in infants and toddlers with DS, a population that has sleep apnea prevalence as high as 50% during the preschool years. Despite poor sleep quality, circadian rhythm and phase were preserved in children with DS and displayed similar developmental trajectories in cross-sectional comparisons with a typically developing (TD) cohort. In line with past work, lower sleep efficiency scores were quantified in the group with DS relative to TD children. Infants born with DS exhibited the worst sleep fragmentation; however, in both groups, sleep efficiency and consolidation increased across age. Three circadian phase markers showed that 35% of the recruitment sample with DS was phase-advanced to an earlier morning schedule, suggesting significant within-group variability in the timing of their daily activity rhythms.
Conclusions: Circadian rhythms of wake and sleep are robust in children born with DS. The present results suggest that sleep fragmentation and any resultant cognitive deficits are likely not confounded by corresponding deficits in circadian rhythms.
Keywords: Actigraphy; Circadian rhythms; Development; Down syndrome; NPCRA (Non-Parametric Circadian Rhythm Analyses); Sleep.
Copyright © 2017 The Author(s). Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
The role of actigraphy in the study of sleep and circadian rhythms.Sleep. 2003 May 1;26(3):342-92. doi: 10.1093/sleep/26.3.342. Sleep. 2003. PMID: 12749557 Review.
-
Circadian phase, sleepiness, and light exposure assessment in night workers with and without shift work disorder.Chronobiol Int. 2012 Aug;29(7):928-36. doi: 10.3109/07420528.2012.699356. Chronobiol Int. 2012. PMID: 22823876
-
Morning Circadian Misalignment Is Associated With Insulin Resistance in Girls With Obesity and Polycystic Ovarian Syndrome.J Clin Endocrinol Metab. 2019 Aug 1;104(8):3525-3534. doi: 10.1210/jc.2018-02385. J Clin Endocrinol Metab. 2019. PMID: 30888398 Free PMC article.
-
Circadian Sleep-Activity Rhythm across Ages in Down Syndrome.Brain Sci. 2021 Oct 25;11(11):1403. doi: 10.3390/brainsci11111403. Brain Sci. 2021. PMID: 34827402 Free PMC article.
-
Circadian Rhythm Sleep-Wake Disorders.Continuum (Minneap Minn). 2017 Aug;23(4, Sleep Neurology):1051-1063. doi: 10.1212/CON.0000000000000499. Continuum (Minneap Minn). 2017. PMID: 28777176 Review.
Cited by
-
Melatonin Relations With Respiratory Quotient Weaken on Acute Exposure to High Altitude.Front Physiol. 2018 Jun 29;9:798. doi: 10.3389/fphys.2018.00798. eCollection 2018. Front Physiol. 2018. PMID: 30008674 Free PMC article.
-
Alterations of specific cortical GABAergic circuits underlie abnormal network activity in a mouse model of Down syndrome.Elife. 2020 Aug 12;9:e58731. doi: 10.7554/eLife.58731. Elife. 2020. PMID: 32783810 Free PMC article.
-
Distribution and age of onset of psychopathological risk in a cohort of children with Down syndrome in developmental age.Ital J Pediatr. 2019 Jul 26;45(1):92. doi: 10.1186/s13052-019-0672-4. Ital J Pediatr. 2019. PMID: 31349869 Free PMC article.
-
Neuronal oscillations in cognition: Down syndrome as a model of mouse to human translation.Neuroscientist. 2025 Jun;31(3):308-325. doi: 10.1177/10738584241271414. Epub 2024 Sep 24. Neuroscientist. 2025. PMID: 39316548 Free PMC article. Review.
-
Influence of Schizophrenia-Associated Gene Egr3 on Sleep Behavior and Circadian Rhythms in Mice.J Biol Rhythms. 2018 Dec;33(6):662-670. doi: 10.1177/0748730418803802. Epub 2018 Oct 15. J Biol Rhythms. 2018. PMID: 30318979 Free PMC article.
References
-
- Fernandez F., Reeves R.H. Assessing cognitive improvement in people with Down syndrome: important considerations for drug-efficacy trials. Handb Exp Pharmacol. 2015;228:335–380. - PubMed
-
- Richtsmeier J.T., Baxter L.L., Reeves R.H. Parallels of craniofacial maldevelopment in Down syndrome and Ts65Dn mice. Dev Dyn. 2000;217:137–145. - PubMed
-
- Donnelly L.F., Shott S.R., LaRose C.R. Causes of persistent obstructive sleep apnea despite previous tonsillectomy and adenoidectomy in children with Down syndrome as depicted on static and dynamic cine MRI. AJR Am J Roentgenol. 2004;183:175–181. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
