

Differentiation of Enhancing Glioma and Primary Central Nervous System Lymphoma by Texture-Based Machine Learning
- PMID: 28450433
- PMCID: PMC7960089
- DOI: 10.3174/ajnr.A5173
Differentiation of Enhancing Glioma and Primary Central Nervous System Lymphoma by Texture-Based Machine Learning
Abstract
Background and purpose: Accurate preoperative differentiation of primary central nervous system lymphoma and enhancing glioma is essential to avoid unnecessary neurosurgical resection in patients with primary central nervous system lymphoma. The purpose of the study was to evaluate the diagnostic performance of a machine-learning algorithm by using texture analysis of contrast-enhanced T1-weighted images for differentiation of primary central nervous system lymphoma and enhancing glioma.
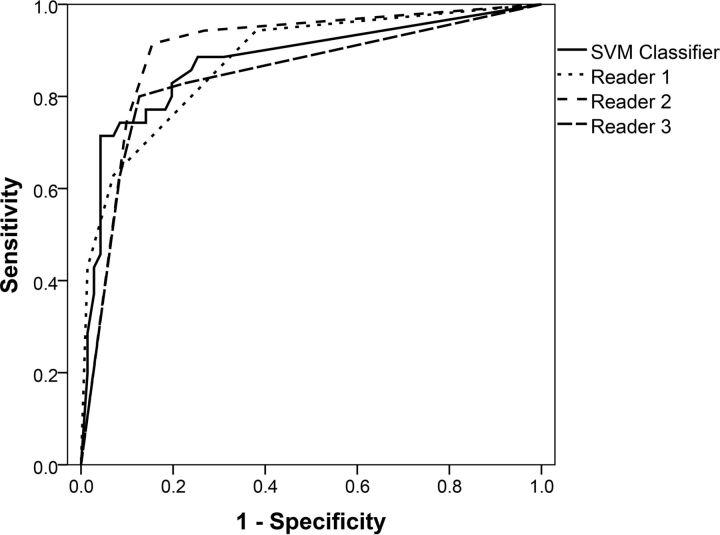
Materials and methods: Seventy-one adult patients with enhancing gliomas and 35 adult patients with primary central nervous system lymphomas were included. The tumors were manually contoured on contrast-enhanced T1WI, and the resulting volumes of interest were mined for textural features and subjected to a support vector machine-based machine-learning protocol. Three readers classified the tumors independently on contrast-enhanced T1WI. Areas under the receiver operating characteristic curves were estimated for each reader and for the support vector machine classifier. A noninferiority test for diagnostic accuracy based on paired areas under the receiver operating characteristic curve was performed with a noninferiority margin of 0.15.
Results: The mean areas under the receiver operating characteristic curve were 0.877 (95% CI, 0.798-0.955) for the support vector machine classifier; 0.878 (95% CI, 0.807-0.949) for reader 1; 0.899 (95% CI, 0.833-0.966) for reader 2; and 0.845 (95% CI, 0.757-0.933) for reader 3. The mean area under the receiver operating characteristic curve of the support vector machine classifier was significantly noninferior to the mean area under the curve of reader 1 (P = .021), reader 2 (P = .035), and reader 3 (P = .007).
Conclusions: Support vector machine classification based on textural features of contrast-enhanced T1WI is noninferior to expert human evaluation in the differentiation of primary central nervous system lymphoma and enhancing glioma.
© 2017 by American Journal of Neuroradiology.
Figures



Similar articles
-
Machine Learning-based Texture Analysis of Contrast-enhanced MR Imaging to Differentiate between Glioblastoma and Primary Central Nervous System Lymphoma.Magn Reson Med Sci. 2019 Jan 10;18(1):44-52. doi: 10.2463/mrms.mp.2017-0178. Epub 2018 May 16. Magn Reson Med Sci. 2019. PMID: 29769456 Free PMC article.
-
Voxel-based clustered imaging by multiparameter diffusion tensor images for glioma grading.Neuroimage Clin. 2014 Aug 7;5:396-407. doi: 10.1016/j.nicl.2014.08.001. eCollection 2014. Neuroimage Clin. 2014. PMID: 25180159 Free PMC article.
-
Primary central nervous system lymphoma and atypical glioblastoma: Differentiation using radiomics approach.Eur Radiol. 2018 Sep;28(9):3832-3839. doi: 10.1007/s00330-018-5368-4. Epub 2018 Apr 6. Eur Radiol. 2018. PMID: 29626238
-
Machine learning applications for the differentiation of primary central nervous system lymphoma from glioblastoma on imaging: a systematic review and meta-analysis.Neurosurg Focus. 2018 Nov 1;45(5):E5. doi: 10.3171/2018.8.FOCUS18325. Neurosurg Focus. 2018. PMID: 30453459
-
Machine Learning in Differentiating Gliomas from Primary CNS Lymphomas: A Systematic Review, Reporting Quality, and Risk of Bias Assessment.AJNR Am J Neuroradiol. 2022 Apr;43(4):526-533. doi: 10.3174/ajnr.A7473. Epub 2022 Mar 31. AJNR Am J Neuroradiol. 2022. PMID: 35361577 Free PMC article.
Cited by
-
Radiomics features to distinguish glioblastoma from primary central nervous system lymphoma on multi-parametric MRI.Neuroradiology. 2018 Dec;60(12):1297-1305. doi: 10.1007/s00234-018-2091-4. Epub 2018 Sep 19. Neuroradiology. 2018. PMID: 30232517
-
Machine learning for semi-automated classification of glioblastoma, brain metastasis and central nervous system lymphoma using magnetic resonance advanced imaging.Ann Transl Med. 2019 Jun;7(11):232. doi: 10.21037/atm.2018.08.05. Ann Transl Med. 2019. PMID: 31317002 Free PMC article.
-
Machine Learning-based Texture Analysis of Contrast-enhanced MR Imaging to Differentiate between Glioblastoma and Primary Central Nervous System Lymphoma.Magn Reson Med Sci. 2019 Jan 10;18(1):44-52. doi: 10.2463/mrms.mp.2017-0178. Epub 2018 May 16. Magn Reson Med Sci. 2019. PMID: 29769456 Free PMC article.
-
A Systematic Review of the Current Status and Quality of Radiomics for Glioma Differential Diagnosis.Cancers (Basel). 2022 May 31;14(11):2731. doi: 10.3390/cancers14112731. Cancers (Basel). 2022. PMID: 35681711 Free PMC article. Review.
-
The effect of CT texture-based analysis using machine learning approaches on radiologists' performance in differentiating focal-type autoimmune pancreatitis and pancreatic duct carcinoma.Jpn J Radiol. 2022 Nov;40(11):1156-1165. doi: 10.1007/s11604-022-01298-7. Epub 2022 Jun 21. Jpn J Radiol. 2022. PMID: 35727458 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical